Valtrex
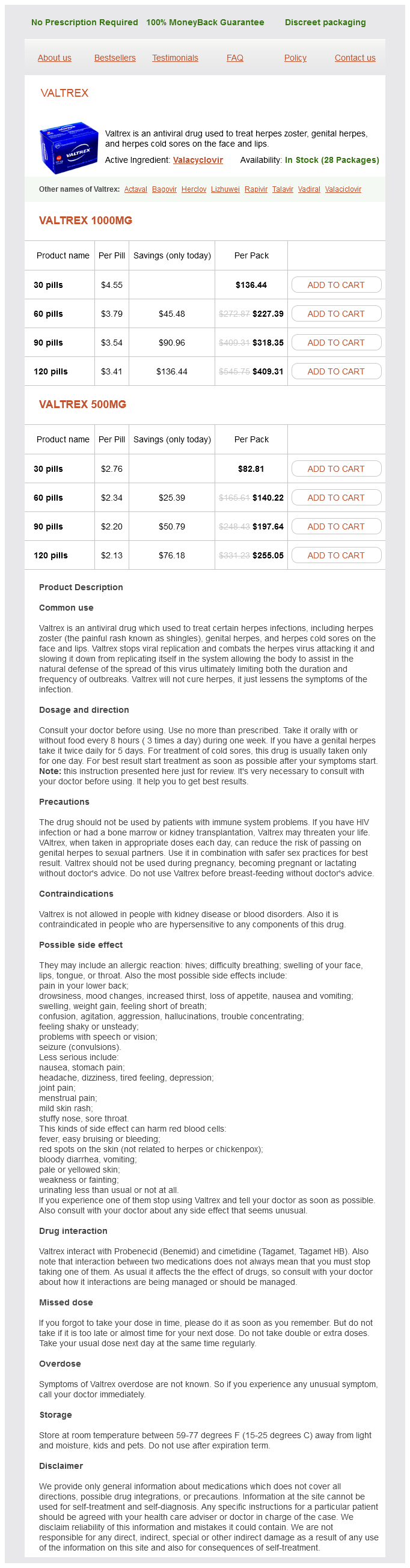
Valtrex 1000mg
- 30 pills - $136.44
- 60 pills - $227.39
- 90 pills - $318.35
- 120 pills - $409.31
Valtrex 500mg
- 30 pills - $82.81
- 60 pills - $140.22
- 90 pills - $197.64
- 120 pills - $255.05
These muscles control the stiffness and intervertebral relationship of the spinal segments and the posture of the lumbar segments hiv infection elderly buy generic valtrex pills. Although this system of muscles is considered essential for stability, it is not sufficient for stability because these muscles are ineffective for control of spinal orientation (Hodges 2004). The global muscle system encompasses the superficial muscles of the trunk that do not have direct attachment to the vertebrae and cross multiple segments. They are considered the torque generators for spinal motion and are said to act as guy ropes to control spinal orientation. These muscles have been shown to balance the external loads applied to the trunk and transfer loads from the thorax to the pelvis (Bergmark 1989). The large variations in external loads that can occur with daily activity are accommodated by the global muscle system so that the resulting load on the lumbar spine and its segments are continually minimized. This makes the global system critical for lumbopelvic stability in terms of spinal orientation, but they cannot fine-tune control of intervertebral motion (Hodges 2004). Cholewicki and others, in a biomechanical in vivo model, found that although the global muscles provided a significant amount of stiffness to the spinal column, activity of the local system was vital in producing stability at the intervertebral/segmental level (Cholewicki et al. Even when forces generated by the global muscles were substantial, the spine was unstable without local muscle activity. Hodges (2004) noted that this local/global muscle system is likely an oversimplification of the complex control of spinal stability; however, it does provide a useful model to consider clinically because evidence suggests that the local muscle system is most impaired in low back pain sufferers even though both systems are seen as necessary to meet the demands of spinal stability (Hodges 2004). Modeling studies (Cholewicki and McGill 1996) suggest that global muscles provide the optimal control of buckling forces, but training those muscles is unlikely to resolve deficits in muscle control. The deep system is seen to provide minimal contribution to control of buckling forces, but it does produce an efficient mechanism to fine-tune the control of intervertebral motion and segments of the pelvis. Finally, the local muscle control is seen to be required over the spectrum of functional demands from light tasks, such as reaching or moving while seated, to the heavier weightlifting tasks. The requirement for strong global muscle action during light tasks is seen as minimal, yet the local system is needed for safe function at the segmental level. Table 8-23 Active Subsystem: the Trunk Muscles Can Be Categorized into Local and Global Muscle Systems Based on Their Architectural Properties local Stabilizing System Intertransversarii Interspinales Multifidus Lumbar part of longissimus thoracis Lumbar part of iliocostalis lumborum Quadratus lumborum, medial fibers Transversus abdominis global Stabilizing System Thoracic part of longissimus thoracis Thoracic part of iliocostalis lumborum Quadratus lumborum, lateral fibers External oblique Internal oblique Rectus abdominis feedforward control of lumbopelvic Stability Lumbopelvic stability is controlled in advance of imposed forces. Studies have demonstrated that activity of the trunk muscles occurs in advance of the muscles responsible for movement of the lower limb (Hodges and Richardson 1997b) and upper limb (Aruin and Latash 1995, Bouisset and Zattara 1987, Hodges and Richardson 1997a) and prior to loading when a mass is added to the trunk in a predictable manner (Cresswell et al. The activity of superficial/global muscles is linked to the direction of forces acting on the spine- that is, superficial trunk muscle activity is earlier and of larger amplitude when the activity opposes the direction of reactive forces (Aruin and Shiratori 2003, Aruin and Latash 1995, Hodges and Richardson 1999). This is consistent with the architectural properties of these muscles to provide a general increase in intervertebral control. Thus, these simple responses are inflexible and represent a basic mechanism for the motor control system to correct an error-resisting an imposed stretch. Some integration of reflexes is seen when reflex changes occur in other related muscles, including contralateral muscles (Beith and Harrison 2004). This suggests that afferent input from distant segments (arm) may be involved in initiation of the trunk muscle response. This also is seen to occur when paraspinal muscle activity is reduced when a load is removed from the trunk by removal of a load from the upper limbs (Hodges et al. Other basic reflex responses have been identified using electrical and/or mechanical stimulation of afferents in ligaments, annulus, facet joint capsule, and sacroiliac joint (Solomonow et al. In general, activity of multifidus was initiated with short latency, on both sides and over multiple segments in response to the applied stimulus. These responses have a longer latency, are more flexible, and can be modified voluntarily. As an example, when the support surface on which a person is standing is rapidly moved, a complex interplay of several body segments, including the trunk, is initiated to maintain equilibrium of the body (Horak and Nashner 1986, Keshner and Allum 1990). Two main strategies have been identified, which involve either ankle motion (ankle strategy) or hip motion (hip strategy), depending on the context and the support surface characteristics (Horak and Nashner 1986). These responses could operate at a simple (short-latency) reflex level or more integrated long-loop reflexes, which involve information processing at higher levels.
Valtrex dosages: 1000 mg, 500 mgValtrex packs: 30 pills, 60 pills, 90 pills, 120 pills
In fact antiviral kleenex purchase cheap valtrex on-line, the patient may seek medical attention repeatedly for what would appear to be physical complaints, as anxiety can effect perception and thought processes. It is commonly expressed in 1050% of those who are suffering from depression [43,44]. The course of anxiety disorders in pregnancy is likely to be related to the severity of the illness preconceptually. The prevalence of generalised anxiety disorder and obsessivecompulsive disorder is higher in the postpartum period than in the general population and over 30% of pregnant women have subsyndromal symptoms of generalised anxiety disorder [43]. Panic attacks and obsessivecompulsive disorder can have enduring biopsychosocial effects on the mother and her infant. Physiological changes in respiratory function during pregnancy can predispose to an increased susceptibility to panic attacks. These can present suddenly as a sense of impending doom, and impair normal functioning. Anxiety, including its exacerbations as panic attacks, can be associated with concerns about the ongoing pregnancy, and its outcome. This can increase the intake of alcohol and substance misuse in those who have been habituated to do so, when facing worrying circumstances prior to pregnancy. Therefore, associated somatic complaints generated by such behaviour could surface. Anxiety may manifest as an obsessivecompulsive disorder, with obsession, compulsion, or both being present simultaneously. Childbearing increases the risk of such behaviour [41], particularly in those with a past history. Often these actions are performed as a ritual or are expressed as mental acts to overcome the intrusions. An acute onset can occur during the puerperium with symptoms escalating within a week, to result in significant maternal distress. Recurring thoughts occur, sometimes about harming the baby, along with repetitive actions to try and avoid these fearful intrusions, and consequently this behaviour contributes to her inability to function normally. Her anxiety can be exacerbated if misinterpreted by her contacts, including those health professionals who are unfamiliar with obsessivecompulsive disorders. The disorder is under-recognised [48,49], despite considerable interference with the maternal role. As with other severe anxiety disorders, motherinfant interaction may be disturbed, with consequent neglect [50]. Tokophobia, from the Greek tokos, meaning birth and phobos, meaning fear, is an unreasonable fear of uterine contractions, and of the vaginal mode of delivery [51]. This could, nevertheless, be aggravated by watching negative portrayals of childbirth [52]. In some individuals, the response to psychosexual adaptation during adolescence may be a contributory factor [53]. In those who were victims of sexual assault it may be initiated by the memory of such an assault. This often follows discussions with peers or after hearing from her mother of a negative childbirth experience. Precipitating factors include an unwanted pregnancy or anxiety about fetal well-being [54]. A need for repeated reassurances from health professionals, along with multiple somatic symptoms induced by pregnancy-related fear that may include panic attacks, can result in an overuse of hospital services to seek reassurance. Paradoxically, in one study, tokophobia occurred in those who had undergone counselling after a traumatic childbirth experience, including caesarean delivery [57]. They may not be willing to accept relevant advice when told that they are not in labour and that an epidural for pain relief is not indicated. Women whose fear of childbirth, following a traumatic birth experience, prevents them from getting pregnant again [20], could benefit from specific psychotherapy [58]. Post-traumatic stress disorder is said to occur when one responds to a traumatic event by expressing fear, helplessness, or horror [59,60]. It manifests as re-experiencing the event with numbing, nightmares, avoidance of reminders of the event, and hyper-arousal, which recur for at least a month [61]. Precipitating social factors include assault or being threatened with death or serious injury [62].
Boron. Valtrex.
- Bone loss (osteoporosis), improving thinking and coordination in older people, and increasing testosterone.
- Are there any interactions with medications?
- Vaginal infections. The most common form of boron called boric acid is applied vaginally for these infections.
- What is Boron?
- Preventing boron deficiency.
- Are there safety concerns?
- How does Boron work?
- Dosing considerations for Boron.
- Body building.
Source: http://www.rxlist.com/script/main/art.asp?articlekey=96861
Partial ruptures occur in well-trained athletes and involve the lateral aspect of the tendon hiv infection fever purchase valtrex 1000 mg on line. The impact of these injuries in athletes is highlighted by the report of Parekh et al. Acute ruptures commonly occur when pushing off with the weightbearing foot while extending the knee, but they also can be caused by a sudden or violent dorsiflexion of a plantarflexed foot (eccentric contracture). Most Achilles tendon ruptures occur approximately 2 to 6 cm proximal to its insertion on the calcaneus, in the so-called "watershed" region of reduced vascularity. Patients should also be questioned about previous steroid injection and fluoroquinolone treatment. Both methods are reasonable, and treatment should be individualized based on operative candidacy. However, the difference in outcomes between conservative and operative treatment is variable. A randomized, prospective study (Twaddle and Poon 2007) found no differences in function, complications, or reruptures between patients treated with or without surgery. Both groups were allowed early controlled motion in a removable orthosis, progressing to full weightbearing at 8 weeks. A large prospective study of 196 patients found a rerupture rate of 7% after 8 weeks of immobilization in a cast or orthosis (Ingvar et al. Partial rupture is associated with an acutely tender, localized swelling that occasionally involves an area of nodularity. If the tendon is ruptured, normal plantarflexion will not occur (a positive Thompson test). In some patients, an accurate diagnosis of a complete rupture is difficult through physical examination alone. A false-negative Thompson test result can occur because of plantarflexion of the ankle caused by extrinsic foot flexors when the accessory ankle flexors are squeezed together with the contents at the superficial posterior leg compartment. Achilles Tendon Rupture 351 nonoperative treatment of Acute Achilles tendon rupture Nonoperative treatment requires immobilization to allow hematoma consolidation. Ultrasound serial examinations are used to confirm that Achilles tendon end apposition occurs with 20 degrees or less of plantarflexion of the foot. Surgical repair is indicated if a diastasis or gap remains with the leg placed in 20 degrees of plantarflexion. Current articles recommend 4 weeks in plantarflexion followed by 4 weeks in neutral or functional rehabilitation in a walking brace after an initial period of 1 to 3 weeks of immobilization. Complications such as adhesions and infection also were more common in the cast immobilization group (36%) than in the functional bracing group (10%). Percutaneous, endoscopically assisted, and mini-open techniques have been developed to speed recovery and improve cosmetic results. Most studies have found lower complication rates with no increase in rerupture rates with percutaneous techniques (Deangelis et al. Percutaneous repair also has been shown to be less costly than open repair (Ebinesan et al. A number of studies have confirmed that physical activity speeds tendon healing, and rerupture rates have not been significantly higher with early weightbearing. A meta-analysis of randomized trials comparing early weightbearing with cast immobilization (Suchak et al. Early functional treatment protocols, when compared to postoperative immobilization, led to more excellent rated subjective responses and no difference in rerupture rated in Suchak et al. Patients in the weightbearing group reported fewer limitations of daily activities at 6 weeks after surgery. At 6 months the surgical group had better results on some of the muscle function tests, but at 12 months the only difference was the heel raise in favor of the surgical group. Functional bracing rather than casting was employed in both groups with improvement of results.
Syndromes
- Endoscopy -- camera down the throat to see burns to the esophagus and the stomach
- Clotting blood
- Muscle weakness that slowly continues to get worse
- Fluids through a vein (IV)
- Sweating
- Procaine
- Brain MRI or CT
- Erythrocyte sedimentation rate (ESR)
The physical tests for the patient having discectomy should aim to provide information that will help guide treatment anti viral enzyme discount 500 mg valtrex fast delivery, such as decreased motor control at the spinal level of the surgery. Based on the list of postoperative disabilities, current best evidence, and clinical experience, the following list of treatments may be seen as a starting point. Furthermore, these neuroscience studies have shown results to extend beyond the short term and to be maintained at 1-year followup. Therapists involved in treating patients who have had discectomy should spend time explaining issues related to the discectomy to the patient. Four broad categories are identified: · Diagnosis: Patients want to know what is going on. A patient should receive information regarding the surgery in a nonthreatening way. A simple explanation of the surgical procedure and issues related to postoperative disability. The therapist should provide information on the plan of care, especially time frames and goals. It may be as simple as explaining that therapy will consist of two visits per week for 4 weeks, at which time a certain disability. The therapists should provide the patient with information regarding at-home instructions. This may include information on limiting sitting, a walking program, application of heat or cold per surgeon guidelines, performing gentle stretches, and more. This is an important part in empowering patients and helping them develop coping strategies. Several studies have shown that fear is a major contributor in the development of persistent pain. Typically the four main issues described are conveyed to the patient during the first visit after Education Education is therapy. Additionally, therapists need to realize that as they embark on the "more physical" part of therapy. Finally, it is also important to realize the role of the acute-care physical therapist. Patients encounter physical therapists in the immediate postoperative period, and although most interactions are brief during gait and transfer training in a typical 1- to 2-day hospitalization after surgery, these interactions can be used as effective means of providing high-quality education. Studies have shown that patients undergoing surgery have increased levels of fear and that educational strategies in or around the time of surgery by health care personnel are effective in decreasing fear. The exact content of the exercise program may consist of spinal stabilization exercises; cardiovascular exercises; general conditioning; and stretches of the lumbar spine, adjacent thoracic spine, and hip joints. It is important to realize that spinal stabilization is motor control, best defined by Hodges (Richardson et al. Rehabilitation Following Lumbar Disc Surgery 495 · · · · · Multifidus should progress to weightbearing exercise. The basis for this is that during weightbearing, local one-joint, stabilizing muscles initiate better and faster compared to open-kinetic chain exercises (Richardson et al. Because stabilization is a motor control activity, focus on repetition, constantly teaching the patient to engage the stabilizers while doing tasks, so that the contractions become automatic. In low back pain the multifidus has been shown to shut down side and level specific and do not spontaneously return after surgery. This further supports the notion of dysfunction in the local stabilizing system after surgery (Gille et al. Even if the surgery resolves the pain, the stabilizing mechanism does not automatically "start up again. Several studies have shown that patients undergoing spinal surgery have high levels of anxiety and fear, which directly affects the spinal stabilizing system. Patients need both spinal stabilization and education to address fear, thus the multimodal approach used in therapy.
Usage: a.c.
Weightbearing · Progress to weightbearing as tolerated with brace locked in full extension hiv infection rate nyc buy valtrex 1000 mg lowest price. Repair of Acute Unilateral Patellar Rupture 303 Repair of Acute Unilateral Patellar Rupture (Continued) · May progress to one crutch on opposite side of involved leg as progressing toward full weightbearing. Range of Motion · 0 to 45 degrees of active knee flexion in hinged knee brace with passive extension in brace. Therapeutic Exercise · Continue quadriceps and gluteal isometrics and patellar mobilizations. Therapeutic Exercise · Open kinetic chain straight leg raise with no extension lag and good vastus medialis obliquus contraction, gluteal strength, short-arc quadriceps, and hamstring curls from 0 to 90 degrees of flexion. Phase 4: Advanced strengthening and functional exercises Weeks 1216 Modalities · Continue with ice if needed for pain and edema. Make sure to check nonsurgical side and upper body for return to sport and activities of daily living. Therapeutic Exercise · Focus should be on balancing muscle strength for control of neutral alignment and beginning sports-specific and functional activity. Continued on following page 304 Knee Injuries Repair of Acute Unilateral Patellar Rupture (Continued) Phase 5: sports-specific drills and Plyometrics Weeks 1624 Modalities · Ice as needed. Closed chain resisted exercises initiated when patient meets criteria for full weightbearing. Weightbearing Weightbearing as tolerated with crutches until patient has full extension, 100 degrees of flexion, no knee extensor lag, and ambulates without pain or effusion. Initiate low-impact aerobic activities (walking program, stationary cycling, swimming) at 3 to 6 weeks, when patient meets full weightbearing status. No open or closed chain resisted exercises for 4 to 6 weeks to avoid loading across the osteotomy site. Osteotomy Touch-down weightbearing for first 2 weeks, partial weightbearing 2 to 4 weeks, weightbearing as tolerated with crutches 4 to 8 weeks. Intermediate Phase (6-12 weeks) Arthroscopic débridement Full motion should be achieved at this time. Agility and sport-specific skill training initiated at 50% effort and progressed to full effort as tolerated. Initiate return to full activity when these activities do not induce recurrent pain or effusion. Muscle Performance Weightbearing Discontinue use of crutches at 6 to 8 weeks when patient has achieved full knee extension, 100 degrees of flexion, and no extensor lag and can ambulate without pain or effusion. May use deweighting device¶ or pool activities in making transition to full weightbearing. Osteochondral grafts Discontinue use of crutches at 6 to 8 weeks when patient has achieved full knee extension, 100 degrees of flexion, and no extensor lag and can ambulate without pain or effusion. May use deweighting device or pool activities in making transition to full weightbearing. Progress to full weightbearing without crutches when patient has achieved full knee extension, 100 degrees of flexion, and no extensor lag and can ambulate without pain or effusion. Low-impact aerobic activities may be initiated when patient achieves full weightbearing status. Continue with progression of resistance for open and closed chain exercises as tolerated in ranges that do not engage lesion site. Functional Retraining and Return to Activity Patients should have returned to full activity by this time period. Agility and sport-specific skill training should be initiated at 50% effort and progressed to full effort as tolerated. May initiate return to activity when tolerating running and agility and sport-specific skill training without recurrent pain or effusion. Initiate agility and sport-specific skill training when tolerating low-impact aerobic activities without recurrent pain or effusion. Osteochondral grafts Osteotomy *Resisted open chain exercises refers to nonweightbearing leg extensions for quadriceps strengthening and leg curls for hamstring strengthening. Resisted closed chain exercises include leg press, partial range squats, wall slides, and step-ups.
References
- Mariappan P, Smith G, Bariol SV, et al: Stone and pelvic urine culture and sensitivity are better than bladder urine as predictors of urosepsis following percutaneous nephrolithotomy: a prospective clinical study, J Urol 173:1610-1614, 2005.
- Bornman, M. S., Franz, R. C., Jacobs, D. J., & Pretorius, H. (1986). Causal relationships between drug-induced hypercoagulability and priapism. Archives of Andrology, 17(3), 231n232.
- Hara T, Inoue Y, Satoh T, et al: Diffusion-weighted imaging of local recurrent prostate cancer after radiation therapy: comparison with 22-core threedimensional prostate mapping biopsy, Magn Reson Imaging 30(8):1091n1098, 2012.
- Goldstein EJ, Citron DM, Merriam CV, et al. Comparative in vitro activities of retapamulin (SB-275833) against 141 clinical isolates of Propionibacterium spp., including 117 P. acnes isolates. Antimicrob Agents Chemother 2006;50:379-81.
- Manson PN, Clifford CN, Su CT, et al. Mechanisms of global support and post-traumatic enophthalmos I. The anatomy of the ligament sling and its relations to intermuscular cone orbital fat. Plast Reconstr Surg 1987;77:193.
- Andrassy RJ, Wiener ES, Raney RB, et al: Progress in the surgical management of vaginal rhabdomyosarcoma: a 25-year review from the Intergroup Rhabdomyosarcoma Study Group, J Pediatr Surg 34:731n734, discussion, 734n5, 1999.