Tadora
Tadora 20mg
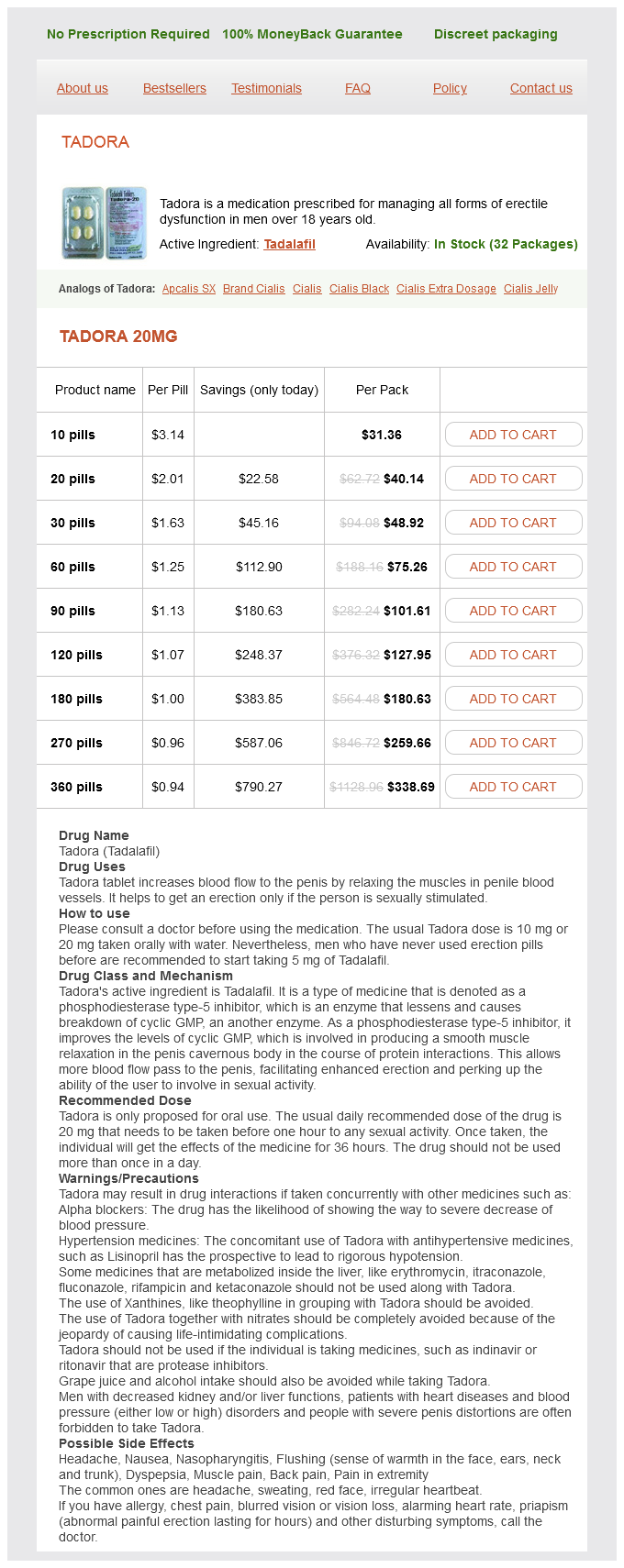
- 10 pills - $31.36
- 20 pills - $40.14
- 30 pills - $48.92
- 60 pills - $75.26
- 90 pills - $101.61
- 120 pills - $127.95
- 180 pills - $180.63
- 270 pills - $259.66
- 360 pills - $338.69
It has also been shown to reduce seizure frequency in supratentorial lesions [103] erectile dysfunction brands tadora 20 mg purchase free shipping. The authors found that sex, age and duration of epilepsy had no prognostic value, but the outcome was better for patients with simple partial seizures than for those with complex partial seizures. Location in the mesiotemporal region was associated with a poor outcome, whereas location in the laterotemporal and central regions was associated with significantly better results. Two reviews from 2007 suggest that the use of radiosurgery over conventional surgery was unproven for epilepsy. Modern dose planning targeting the lesion only (and not the adjacent brain) with lower doses has reduced the complication rate but whether this has altered clinical outcome is not known. Excellent results have been reported for the treatment of mesial temporal lobe epilepsy associated with hippocampal sclerosis by gamma knife [111,112]. Although further evaluation of effects of radiosurgery on seizures associated with cavernous malformation is necessary, this form of treatment may be useful for intractable epilepsy related to lesions situated in eloquent or inaccessible areas of the brain. Intracranial aneurysms Epilepsy is an extremely uncommon presentation of intracranial aneurysm. Although seizures are a well-recognized presentation of subarachnoid haemorrhage, we refer specifically to unruptured intracranial aneurysms causing epilepsy through mass effect on adjacent brain. Although not well recognized, it is described in case reports with cessation of seizures coinciding with aneurysm ablation. Aneurysms presenting in this way are likely to involve the middle cerebral artery and/or exert mass effect on the medial temporal structures, giving rise to complex partial seizures [113,114]. They represent the most commonly documented intracranial vascular malformation by either brain imaging or autopsy, with a prevalence as high as 3% [115]. Angiography typically shows a caput medusae appearance in the late venous phase [117]. In a prospective study of 80 patients the bleeding rate per year was calculated to be 0. Resection of these lesions is generally associated with high morbidity and mortality [122,123,124], probably because the venous anomaly is a functioning venous channel that drains normal parenchyma and surgical removal of such channels can thus lead to venous infarction [118]. Similarly, radiosurgery is thought to carry a 30% risk of radiation complications or venous infarctions and may not achieve total obliteration [125]. Capillary telangectasias Capillary telangectasias are often detected as incidental findings at autopsy. They appear as poorly demarcated pink or reddish discoloured lesions with dilated capillaries and may look like a petechial haemorrhage. The intervening parenchyma between the vessels is usually normal and gliosis and microhaemorrhages are absent, distinguishing these anomalies from other vascular malformations [126]. These lesions are extremely rare: in a series of 30 000 autopsies, capillary telangiectasias were identified in 0. These malformations are usually seen in hereditary haemorrhagic telangiectasias (including OslerWeberRendu syndrome), or associated with other vascular anomalies such as cavernous angiomas. The usual presentation of symptomatic lesions is haemorrhage or epilepsy and in a study of 21 patients, seizures occurred in nine cases and haemorrhage in eight [129]. Typical appearances include a variable T1 appearance, high signal intensity on T2-weighted images, contrast enhancement and a lack of mass effect. Haemorrhage and calcifications are rare, suggesting that the findings on T2-weighted images are probably related to the presence of deoxyhaemoglobin in slow-flowing blood. Although seizures may be present in a high percentage of these [123], the number of reported cases is so small that it is likely that these are incidental findings during epilepsy investigation. The absence of cases reported in the literature does not allow us to draw any firm conclusions as to the epileptogenic or bleeding potential of capillary malformations and on the strength of currently available medical evidence, the discovery of one or more of these lesions during investigations for epilepsy or haemorrhage should not alter the routine surgical or medical management of the underlying pathology. Abscess secondary to paranasal sinusitis commonly occurs between 10 and 30 years of age, 25% occurring in children below 15 years. Predisposing factors Brain abscess can develop by direct extension of infection into the brain (this includes trauma and surgery) or by haematogenous spread from remote regions of the body. The most common cause was direct extension from the paranasal sinuses or ear but with more effective antibiotic treatment of sinus infections, haematogenous spread is now the most common cause. Direct spread Chronic middle ear infection is the most common cause of direct intracranial spread (acute infection rarely spreads intracranially). Cholesteatoma is an additional risk factor, increasing the incidence of intracranial extension from 23. Brain abscesses related to middle ear infection are usually solitary, arising in the inferior temporal lobe adjacent to the petrous temporal bone.
Tadora dosages: 20 mgTadora packs: 10 pills, 20 pills, 30 pills, 60 pills, 90 pills, 120 pills, 180 pills, 270 pills, 360 pills
Carbon-tipped surface electrodes are placed on the exposed regions of temporal and suprasylvian neocortex impotence quotes the sun also rises safe tadora 20 mg. Our practice is to pursue a total hippocampal removal, assuming that our preoperative multivariate analysis of neuropsychological, imaging and electrographic parameters predicts a favourable outcome with regard to verbal memory [18]. Hemispheric specialization for emotional expression: A reexamination of results from intracarotid administration of sodium amobarbital. Severe behavioral complications following intracarotid sodium amobarbital injection: implications for hemispheric asymmetry of emotion. Severe negative emotional reactions in intracarotid sodium amytal procedures: further evidence for hemispheric asymmetries Emotional outbursts and post-traumatic stress disorder during intracarotid amobarbital procedure. Does the intracarotid amobarbital procedure predict global amnesia after temporal lobectomy The intracarotid amobarbital procedure as a predictor of memory failure following unilateral temporal lobectomy. Intraoperative hippocampal electrocorticography to predict the extent of hippocampal resection in temporal lobe epilepsy surgery. Language dominance in children as determined by magnetic source imaging and the intracarotid amobarbital procedure: a comparison. An update on determination of language dominance in screening for epilepsy surgery: the Wada test and newer noninvasive alternatives. Weighing the value of memory loss in the surgical evaluation of left temporal lobe epilepsy: A decision analysis. Naming ability after tailored left temporal resection with extraoperative language mapping: increased risk of decline with later epilepsy onset age. Electrocorticographic functional mapping identifies human cortex critical for auditory and visual naming. Presurgical motor and somatosensory cortex mapping with functional magnetic resonance imaging and positron emission tomography. The anesthetic considerations of intraoperative electrocorticography during epilepsy surgery. A retrospective analysis of a remifentanil/propofol general anesthetic for craniotomy before awake functional brain mapping. A comparison of effects of alfentanil, fentanyl, and remifentanil on hemodynamic and respiratory parameters during stereotactic brain biopsy. The role of the alpha2-adrenoceptor agonist dexmedetomidine in postsurgical sedation in the intensive care unit. Correlation and linear regression between blood pressure decreases after a test dose injection of propofol and that following anaesthesia induction. Bispectral index monitoring during sedation with sevoflurane, midazolam, and propofol. The analgesic action of dexmedetomidinea novel alpha 2-adrenoceptor agonist-in healthy volunteers. A comparison of the sedative, hemodynamic, and respiratory effects of dexmedetomidine and propofol in children undergoing magnetic resonance imaging. Comparison between dexmedetomidine and propofol for sedation in the intensive care unit: patient and clinician perceptions. Extent of medial temporal resection on outcome from anterior temporal lobectomy: a randomized prospective study. The predictive value of intraoperative electrocorticography in resections for limbic epilepsy associated with mesial temporal sclerosis. Dysnomia after left anterior temporal lobectomy without functional mapping: frequency and correlates. Left temporal neocortex mediation of verbal memory: evidence from functional mapping with cortical stimulation. The goal of surgical treatment is to eliminate seizures as quickly and early in brain development as possible while minimizing adverse effects. Seizure control early in cerebral development is important to ensure optimal cognitive and functional outcomes [1]. In this chapter, the concepts of paediatric epilepsy surgery are reviewed with an emphasis on literature published in the last 10 years. The chapter starts with an appraisal of treatment-resistant epilepsy and emphasizes the neurodevelopmental consequences of suboptimal seizure control. This is followed by the presurgical evaluation and surgical management of patients with paediatric epilepsy. Finally, an analysis of surgical outcomes with regards to seizure control, complications, cognitive development and quality of life is described.
Beta-1-6,1,3-Beta-Glucan (Beta Glucans). Tadora.
- What other names is Beta Glucans known by?
- Dosing considerations for Beta Glucans.
- Lowering cholesterol levels when taken by mouth.
- Are there any interactions with medications?
- What is Beta Glucans?
Source: http://www.rxlist.com/script/main/art.asp?articlekey=96996
How then does a primary care physician decide to treat patients with features of both However erectile dysfunction treatment ppt tadora 20 mg purchase with visa, the discharge note advised the primary care physician to repeat the spirometry after a period of 6 weeks following the acute episode. Sadly, this man died mowing his lawn a few months later, and the postmortem found severe macroscopic bronchiolar mucous plugging and thickened basement membrane on histology of the lungs. Comment: Fixed airflow (irreversible) obstruction may occur in people with longstanding or severe asthma, and it is important to establish from the medical history whether older people with respiratory problems had symptoms in their youth. Someone with childhood asthma can exhibit ongoing respiratory symptoms without reporting these to the doctor. As a result, chronic asthma with fixed airflow obstruction can persist, and patients may tolerate the symptoms without complaining to their doctor. In the case of chronic obstructive lung diseases, the respiratory literature is peppered with studies demonstrating that many patients are treated on the basis of an uncorroborated clinical diagnosis. This idea, while welcomed by primary care colleagues (personal communications), has generated widespread debate among specialists. It is de ned by the history of respiratory symptoms such as wheeze, shortness of breath, chest tightness, and cough that vary over time and in intensity, together with variable expiratory air ow limitation. Exacerbations and comorbidities contribute to the overall severity in individual patients. Alternatively, someone with a history of atopy or allergy, a family history of asthma and allergy, and whose chronic intermittent respiratory symptoms started before the age of 30, probably has asthma. Often triggered by exercise, emotions (including laughter), dust, or exposure to allergens Current and/or historical variable air ow limitation. Neutrophils ± eosinophils in sputum, lymphocytes in airways, may have systemic in ammation Persistent air ow limitation Frequently a history of doctordiagnosed asthma (current or previous), allergies, a family history of asthma, and/or a history of noxious exposures Symptoms are partly but signi cantly reduced by treatment. Patients can bene t from reference to an experienced asthma educator to obtain essential information and teach self-management skills, if available. Education takes time, and the busy clinicians are not always able to provide this type of intervention. Enabling patients with knowledge and emergency supplies of medication for initiating treatment for exacerbations is important, not only because they may have di culty accessing medical care early enough, but also to try and abort the attacks and prevent hospitalization. A typical self-management emergency pack for asthma usually includes oral corticosteroid tablets, an extra short-acting bronchodilator inhaler, and a peak- ow meter to monitor progress. In all cases, patients should be taught to seek medical assistance soon a er initiating these medications, mainly so the clinician can assess the severity and progress of the attack, to establish whether there were any preventable factors preceding the attack, and so that treatment and preventative measures can be optimized according to local guidelines. Simply treating patients for acute are-ups or exacerbations without recognizing these issues signify failure of treatment, is insu cient. Following initial diagnosis and treatment, and a er approximately 6 to 8 weeks or sooner following treatment for an acute attack. A er the initial diagnosis, further testing that could be arranged should include the following: 23. As the test results are used as a basis for diagnosis and selection of therapy options, it is essential these are performed by trained individuals, and must be of a high standard for quality assurance. As normal lung function may be present at times, by de nition, in the people with asthma, it is not practical in primary or specialist practice, to perform serial spirometry investigations in those with a suggestive clinical history. Patients are managed predominantly in primary care, and specialist assistance is sought for diagnosis and intermittently for emergency management. Given recent reports of poor outcomes, and marked variability in standards of care and outcomes,34 perhaps it is time to rethink the way chronic respiratory disease is managed. One suggestion pertaining to asthma includes35 specialists providing outreach community clinics. For example, a scheme in the northern Netherlands where patients with suspected obstructive lung disease are referred from primary to secondary care specialists, who then provide a remote-access advisory service on diagnosis and management. In some countries, such as the United Kingdom, chronic disease review is delegated to nurses or health-care assistants, who utilize a pro-forma checklist for doing the review. Asthma control assessment includes two main components: current symptom control, which is assessed using presence of symptoms plus the patients need for reliever medication, and risk factors for future attacks. If the patient has poor current control, medication or the device may need changing.
Syndromes
- Coma
- Lymph node biopsy and culture
- Family member who committed suicide
- Cerebral infarction (stroke)
- Colonoscopy
- Abdominal pain
In general erectile dysfunction and diabetes leaflet discount 20 mg tadora otc, postoperative wound infections and haemorrhages seem to have the same low incidence as with other neurosurgical procedures of similar extent and duration and will deserve the same prophylactic and therapeutic measures. Seizure outcome will depend primarily on the underlying pathology and is inferior in patients with extensive malformations of cortical development, including hemimegalencephaly. In our own experience with the vertical parasagittal hemispherotomy, as well as that of other neurosurgeons with the lateral approach hemispherotomy, overall surgery-related morbidity and hospital stay are significantly reduced, due to a very limited amount of cerebral tissue removal, a shorter length of the surgical procedure and a reduced amount of blood loss. Once the hemispheric resection or disconnection is supposed to be complete, a failure to control seizures is most probably due to epileptogenic tissue within the remaining opposite hemisphere. The timing of surgery depends primarily on factors such as duration and severity of the seizure disorder, dynamic evolution of the disease, and actual neurological and cognitive state. Particularly in children with malformations of cortical development and with Rasmussen encephalitis of the language-dominant hemisphere, the decision when to operate remains a challenge, in order to achieve the best possible long-term cognitive development, degree of autonomy and quality of life. Conclusion When unilateral hemispheric refractory epilepsy has been well documented, including a meticulous analysis of the integrity of the 1. Removal of right cerebral hemisphere for certain tumors with hemiplegia: Preliminary report. Cerebral hemispherectomy in pediatric patients with epilepsy: comparison of the three techniques by pathological substrate in 115 patients. Epilepsy surgery for hemispheric syndromes in infants: hemimegalencephaly and hemispheric cortical dysplasia. Treatment of Rasmussen encephalitis half a century after its initial description: Promising prospects and a dilemma. Activation of the remaining hemisphere following stimulation of the blind hemifield in hemispherectomized subjects. Unconscious vision: new insights into the neuronal correlate of blindsight using diffusion tractography. Distinct right frontal lobe activation in language processing following left hemisphere injury. Language recovery after left hemispherectomy in children with late-onset seizures. Exceptional verbal intelligence after hemispherotomy in a child with Rasmussen encephalitis. Cerebral hemispherectomy: hospital course, seizure, developmental, language, and motor outcomes. The role of hemispherectomy in the treatment of holohemispheric hemimegalencephaly. The outcome of 58 children after hemispherectomy: the Johns Hopkins experience: 19681996. Functional hemispherectomy for treatment of epilepsy associated with hemiplegia: rationale, indications, results, and comparison with callosotomy. Anatomical hemispherectomy for intractable seizures: excellent seizure control, low morbidity and no superficial cerebral hemosiderosis. It was first performed 75 years ago by Van Wagenen and Herren [1], who had observed that patients sustaining stroke or tumour progression destroying the corpus callosum often had improvement in an associated seizure disorder. There was laboratory evidence supporting the rationale for this procedure, notably that of Erickson [2], who in non-human primates demonstrated prevention of the spread of the epileptic discharge to the opposite hemisphere when the corpus callosum had been divided. Following this early work, a small number of clinical series were reported [3,4,5,6,7,8,9,10,11,1 2,13,14,15,16,17,18,19,20,21,22], but it was not until the late 1980s that the procedure was widely adopted as a surgical option for medically intractable epilepsy patients who were not candidates for resective procedures. Today, most epilepsy centres perform commissurotomy, and it retains an important role in the armamentarium of interventions for intractable epilepsy. Indications Although resection of an epileptogenic region with the goal of surgical cure has always been the surgical procedure of choice, in those patients with generalized seizures in whom a discrete epileptogenic region cannot be identified or resected, surgical disruption of secondary generalization is a reasonable option. Other palliative procedures, including multiple subpial transection, vagal nerve stimulation and deep brain stimulation, have also been developed, and the strategy for optimal utilization or prioritization of these various non-ablative strategies remains to be determined [23,24,25]. From the earliest days of callosotomy it has been appreciated that drop attacks (variously classified as atonic and akinetic seizures) are among the most likely of seizure types to benefit from disconnection; tonic and tonicclonic generalized seizures similarly have been shown to be significantly reduced [14,15,21,24,25,26,27,28,29, 30,31,32,33,34,35,36,37,38,39,40,41,42,43,44,45,46,47,48,49,50,51, 52,53,54,55,56,57,58,59,60,61,62,63,64,65,66,67,68,69,70,71,72,73, 74,75,76,77,78,79,80,81,82,83,84,85,86,87,88,89,90,91,92,93]. Given the difficult evaluation in this patient population, it is both understandable and reasonable that many patients have undergone callosal section largely on the basis of their seizure semiology.
Usage: p.r.n.
Presurgical evaluation Finding an intracerebral lesion in a patient with recurrent seizures does not necessarily mean that this structural abnormality is producing the seizure activity can erectile dysfunction cause low sperm count purchase cheap tadora on-line. The main purpose of the presurgical evaluation in patients with intracranial lesions and intractable seizures is to confirm the relationship between the lesion and the seizure foci. In some patients, the epileptogenic focus is contiguous with but extends beyond the structural lesion [11,12,13,14]. The lesion may occasionally be incidental and bear no causal relationship to the epileptogenic focus. Therefore, the understanding of spatial and causal relationship between structural lesions of the brain and intractable epilepsy is essential in planning therapeutic strategies. The preoperative evaluation in patients with Resective surgery of neoplasms 847 the most frequent seizure type associated with lesional epilepsy is the complex partial seizure. Seventy-five per cent of patients with temporal lobe lesions had typical temporal lobe seizures [12]. An equally good correlation was shown in patients with frontal and occipital lobe lesions but not in patients with parietal lobe lesions. Seizures originating in the parietal lobe can mimic frontal and temporal lobe seizures [80]. A change in seizure frequency was not found to be a reliable indicator of a cerebral neoplasm. However, after successful treatment, return of seizures has been an indicator of tumour recurrence that may not be detected radiologically for several months [11,12]. History and examination A careful history should be taken in all patients with seizures, with particular attention to a history of febrile seizures, developmental milestones, head trauma and previous neurological problems. Sixteen per cent of the patients with space-occupying lesions and intractable epilepsy had a positive family history of epilepsy, which may indicate an increased susceptibility to seizures in these patients. A thorough neurological examination can detect abnormalities such as a mild hemiparesis or visual field defect that may assist in clinically lateralizing the epileptogenic zone. Facial weakness, especially during emotional expression, may occur in patients contralateral to the epileptic temporal lobe and is uncommon in normal subjects [81,82]. However, since a majority of the lesions are small and are detected on imaging before any gross mass effect appears, clinical examination is non-contributory in most of these patients. Age at onset of seizures Although earlier studies found a low incidence of tumours in patients with onset of seizures before the age of 20 years [83,84], more recent data suggest that refractory focal seizures, even before the age of 20, should raise suspicion of an intracranial mass lesion [11,12]. Among a group of 27 patients with intracranial mass lesions and medically refractory focal epilepsy, age at onset of seizures was the same for neoplastic and non-neoplastic lesions [11]. Routine electroencephalogram recording Structural lesions are now most often recognized on neuroimaging and most patients undergoing surgery are undergoing resections of the lesion because the extent of resection of the structural abnormality is the most consistent and important prognostic factor for seizure control [12,14]. The occurrence of interictal focal sharp and/ or focal slow activity in patients with an intracranial space-occupying lesion has been extensively documented [85]. The absence of prominent focal slow-wave activity in this patient population is mainly due to the limited circumscribed character of most of these lesions. However, when present, a unilateral focal interictal abnormality was a reliable predictor of the side of the lesion. The spatial distribution of the focus coincided with the lesion localization in only 30% of the patients, especially with occipital lesions [87,88]. Patients with temporal lobe lesions were not significantly more likely than extratemporal patients to have an ipsilateral temporal spike or sharp wave focus. Poor interictal scalp localization has been attributed to the fact that the recorded focal abnormality may only be a part of a deeply localized, more extended focus that propagates to the surface. The occurrence of bilateral independent sharp waves and spikes in patients with epilepsy has been well recognized [89,90,91]. In the absence of a detectable lesion, this finding can lead to a decision not to operate on a patient with intractable focal seizures. Neuroimaging Advanced neuroimaging is arguably the most important aspect of the presurgical evaluation of patients with lesional epilepsy because it provides information about the exact location and extent of the lesion [16]. The diagnostic yield of the neuroimaging studies depends on the underlying pathology and the anatomical localization of the epileptogenic area. The selection of patients for epilepsy surgery, the presurgical evaluation and the surgical strategy will be greatly influenced by the neuroimaging-identified lesion [11,12,13,14].
References
- Hendren WH: Urinary undiversion: refunctionalization of the previously diverted urinary tract. In Walsh PC, Retik AB, Vaughan ED Jr, et al, editors: Campbellis urology, Philadelphia, 1998, Saunders, p 3247.
- Suzui H, Hoshimaru M, Takahashi JA, et al. Immunohistochemical reactions for fibroblast growth factor receptor in arteries of patients with moyamoya disease. Neurosurgery 1994;35:20.
- Poplin E, Feng Y, Berlin J, et al. Phase III, randomized study of gemcitabine and oxaliplatin versus gemcitabine (fixed-dose rate infusion) compared with gemcitabine (30-minute infusion) in patients with pancreatic carcinoma E6201: a trial of the Eastern Cooperative Oncology Group. J Clin Oncol 2009;27(30):3778-3785.
- doi:10.1016/j.ejphar.2008.