Plendil
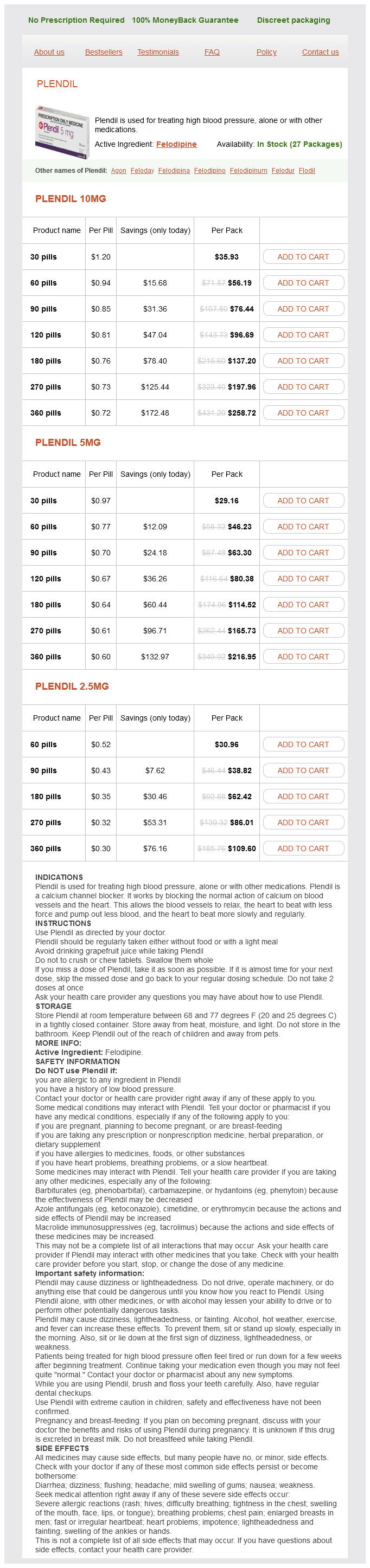
Plendil 10mg
- 30 pills - $35.93
- 60 pills - $56.19
- 90 pills - $76.44
- 120 pills - $96.69
- 180 pills - $137.20
- 270 pills - $197.96
- 360 pills - $258.72
Plendil 5mg
- 30 pills - $29.16
- 60 pills - $46.23
- 90 pills - $63.30
- 120 pills - $80.38
- 180 pills - $114.52
- 270 pills - $165.73
- 360 pills - $216.95
Plendil 2.5mg
- 60 pills - $30.96
- 90 pills - $38.82
- 180 pills - $62.42
- 270 pills - $86.01
- 360 pills - $109.60
I never knew anyone who had any type of brain tumor heart attack 21 year old female buy plendil 2.5 mg line, so it seemed, at times, that I was going through this alone. Coming to the support group allowed me to meet people who also had a vestibular schwannoma. There were many others out there who shared similar problems to mine, and we were bonded on that basis. Together, we can make a difference for others who are newly diagnosed and those who have difficulty dealing with their present reality. However, some may enlarge much more rapidly, and yet others may actually involute. Growth patterns may be characterized by saltatory growth, linear growth, exponential growth, stable size, and decreasing size. There is a common belief that after growth is witnessed, most tumors will continue to grow indefinitely. However, this notion is easily discredited by the simple observation that many tumors do not grow for extended periods following diagnosis, but of course, the tumor must have grown at some point to reach its current size. Not surprisingly, the proportion of growing tumors seems to increase with longer follow-up. Overall, a hearing preservation rate of approximately 50% during a mean follow-up period ranging from 2 to 5 years is to be expected. Each modality has pros and cons, and several factors have to be taken into account when advising patients about treatment options. For patients with small tumors and mild or no symptoms, the controversy is especially pointed. According to the Hippocratic Oath, treatment should not cause more morbidity to the patient than the natural course of the disease, neither in the short or long term. Therefore, it is most important to have a thorough knowledge about the natural course of the disease, both regarding tumor growth, QoL, and symptom development. The dilemma in patients with small tumors and good ipsilateral hearing is to evaluate the treatment choice regarding chance of hearing preservation and tumor control, both immediately and in the long term. There are different follow-up algorithms regarding imaging intervals and duration of follow-up needed. Most authors recommend the first scan 6 months after the initial scan to identify rapid growing tumors. Several authors recommended conservative treatment, or no treatment, for most small tumors with minor or no complaints. This risk needs to be compared with the likelihood of preserving hearing if the tumor is treated by surgery or radiosurgery. These results may be biased by the fact that observed tumors were not growing and that larger tumors tended to receive microsurgical resection. Tumor growth is usually defined as linear increase or tumor volume doubling time, but growth of intrameatal tumors to extrameatal extension is also used. The efficacy of conservative treatment, as defined as freedom from active treatment, is reported in several studies. Hearing preservation is reportedly achieved in about 50 to 70% of selected cases, with extreme good results (100%) in one series. The literature on this topic is largely characterized by single institution, even single-surgeon series-and there are likely tremendous inclusion and treatment biases. With a tumor margin dose of 13 Gy, 60 to 75% serviceable hearing preservation is reported with a mean follow-up period of 3 to 5 years. So far, we do not know for certain if radiosurgery protects or aggravates hearing loss. Sensitivity tests and threshold analyses showed that observation followed by radiosurgery gave the best QoL value until a hearing loss exceeds 12. The microsurgical group sensitivity analyses failed to reach significant thresholds. If careful monitoring of tumor size and hearing level show changes, definitive treatment should be considered. The best way of preserving serviceable hearing as long as possible might therefore be observation, eventually followed by radiosurgery. Sudden sensorineural hearing loss as a revealing symptom of vestibular schwannoma. Conservative management of acoustic neuroma: a meta-analysis and proposed treatment algorithm.
Plendil dosages: 10 mg, 5 mg, 2.5 mgPlendil packs: 30 pills, 60 pills, 90 pills, 120 pills, 180 pills, 270 pills, 360 pills
When properly applied pulse pressure formula plendil 10 mg overnight delivery, the procedure is associated with unmistakably slow systemic drug absorption due, largely, to preferential lidocaine partitioning into fatty tissues prior to suctioning (250). Klein indicated 35 mg/kg as a conservative estimate of the safe maximum dose, based on the observation of Cmax values well below the toxic threshold at 10 to 15 hours after injection (251). He emphasized the use of a dilute solution with added epinephrine, injected slowly over 45 minutes, whereas injection of large doses over less than 5 minutes results in dangerously rapid drug absorption. Up to about 90% of the dose of lidocaine is absorbed, and up to 30% of the dose is recovered with the removal of the subcutaneous fat tissue (251,252). It has been confirmed that epinephrine (1:1,000,000) significantly retards the absorption of lidocaine administered by the tumescent technique and may allow time for some lidocaine to be removed from the tissues by suction lipectomy (253). Moreover, the high pressure generated in the subcutaneous tissues during injection of the solution does not affect the absorption of lidocaine (253). Regardless of the rate of absorption, a local anesthetic with a rapid local and systemic metabolism presents a more appealing strategy for avoiding systemic toxicity, and recent studies suggest that articaine may be useful in this role (254). Direct instillation of longer-acting local anesthetics into wounds is currently receiving attention corresponding to the availability of multiport catheters and elastomeric infusion devices that regulate the rate of infusion through controlled contraction of the reservoir. The local anesthetic agent is thereby placed into a milieu of mixed tissues with a possibility of both rapid absorption and depot formation. The range of ropivacaine concentrations was quite large, approaching some values of concern for toxicity in these patients; however, the unbound concentrations decreased concurrently, presumably the consequence increases in 1 -acid glycoprotein induced by surgery, and this was seen by the authors to confer a safety factor. Intra-articular injection of local anesthetic agents for pain management after arthroscopic surgery has been found efficacious in some studies, but not in others: Dose and timing seem Chapter 3: Properties, Absorption, and Disposition of Local Anesthetic Agents 69 Dosage Factors Concentration and Volume All other things being constant, total dose is the primary determinant of drug plasma concentrations after any route of perineural administration. However, it must be remembered that the drugs are not inert tracers so that their pharmacologic effects, including the neural blockade produced, can also provoke deviations or nonlinearities in their pharmacokinetics, particularly when the local concentration of drug approaches toxic levels or saturation levels for some transport or metabolic binding process. For example, plasma Cmax after caudal doses of ropivacaine 1, 2, or 3 mg/kg in children were found to be proportional to dose, but with a tendency toward decreasing Tmax with increasing dose (263). Likewise, given up to a 300-mg epidural dose (constant volume) of etidocaine, plasma concentrations increase linearly with dose, but beyond this they become disproportionately higher (264). These differences presumably reflect saturation of local binding sites and/or greater vasodilator effects produced by more concentrated solutions. Both of these mechanisms should result in disproportionate increases in plasma drug concentrations when concentration and mass of drug are increased but volume is held constant. Plasma lidocaine levels in a subject following cuff release after intravenous regional anesthesia with 3 mg/kg lidocaine (0. There is no systemic absorption process as for perineural injections, although there is a systemic resorption process of drug that diffuses into local tissues during cuff inflation. This is consistent with the observation that only about 12% of the dose can be aspirated from veins shortly after injection. The bulk of the dose remains in arm tissue, with 50% remaining in the limb 30 minutes after cuff release (170). Intermittent deflation of the cuff for 10 to 30 seconds followed by reinflation appears to have little effect on the ultimate maximum plasma drug concentration but does prolong the time to maximum concentration (260). Prior logic suggested that prilocaine best filled this role for anesthe- Speed of Injection It is intuitive that a slower rate of drug administration conveys greater safety than a faster one for a neural blockade procedure. Emphasis on safety improvements in regional anesthesia has led to the practice of dose fractionation for avoiding toxicity, whereby the dose is administered slowly or as a series of increments. Epidural injections given over 1 minute resulted in 16% higher maximum plasma concentrations of lidocaine compared with those injected in 15 seconds (266). Plasma bupivacaine concentrations were not influenced by varying epidural injection speed from 20 to 100 seconds (215). Various comparative studies with articaine, prilocaine, and lidocaine indicate that articaine can produce a faster onset with a briefer duration than lidocaine, but its circulating concentrations are much smaller than lidocaine due to extensive local hydrolysis prior to tourniquet release combined with its rapid clearance from the plasma post-tourniquet release (12,261,262). The concern of a dose mistakenly being administered intravenously was investigated in sheep, where it was found that prolonging administration of 37. The authors suggested that the most important feature of dose fractionation is that it gives the anesthesiologist an early opportunity to cease administering the drug if an adverse effect is detected.
Mushroom (Agaricus Mushroom). Plendil.
- Are there safety concerns?
- Chemotherapy side effects. Preliminary research suggests that taking agaricus mushroom might reduce some of the side effects of chemotherapy. But this research is too preliminary to use agaricus mushroom for this purpose.
- What is Agaricus Mushroom?
- How does Agaricus Mushroom work?
- Dosing considerations for Agaricus Mushroom.
- What other names is Agaricus Mushroom known by?
Source: http://www.rxlist.com/script/main/art.asp?articlekey=97109
Local anesthetics have actions on coagulation heart attack exo lyrics buy 10 mg plendil visa, inflammation, immune responses, and inbibit a wide variety of enzymes and receptors (71). There is even provocative new evidence that systemically administered lidocaine shortens length of stay and improves outcomes after surgery (72). A nearly unique systemic side effect of prilocaine is its doserelated ability to initiate methemoglobinemia (73,74). The historic "dogma" was that doses of prilocaine must exceed 600 mg before clinically important fractions (>5%) of methemoglobinemia would appear in adults (4,5). Recent studies suggest that clinically important concentrations (>10%) may occur with prilocaine doses as small as 400 mg in otherwise healthy young adults (75). The formation of methemoglobin is believed to be related to the degradation of prilocaine in the liver to o-toluidine, which converts hemoglobin to methemoglobin (73). Although mild degrees of methemoglobinemia are of little clinical importance in most patients with normal oxygen-carrying capacity, this complication has limited the use of this otherwise potentially valuable drug. Dangerous degrees of methemoglobinemia are more commonly associated with benzocaine than prilocaine, at least in American hospitals (76). In surgical patients, one should be cognizant that dangerous levels of methemoglobin may result from treatment with dapsone (used for opportunistic infections in the immunosuppressed), dehydration, and 20% benzocaine spray used for topical anesthesia (Table 4-3). Note that comparisons of all of the agents at "equally effective" concentrations and under the same conditions have not been made in humans. Peripheral Vascular Effects Local anesthetics exert a biphasic action on smooth muscle of peripheral blood vessels related to inhibition of nitric oxide mechanisms and vasoconstriction at very reduced concentrations and vasodilation at clinical concentrations (8,9). For example, exposure of arterioles in the cremaster muscle of rats to concentrations of lidocaine of 10 to 1,000 g/mL produced a dose-related state of vasoconstriction varying from 88% to 60% of the control vascular diameter (9). An increase in the concentration of lidocaine to 10,000 g/mL produced approximately a 27% increase in arteriolar diameter, indicating a significant degree of vasodilation. Other studies using an isolated rat portal vein preparation have also demonstrated that local anesthetic drugs vasoconstrict at reduced concentrations and inhibit myogenic activity at increased concentrations (8). Allergic Effects Many patients report histories suggestive of allergic or hypersensitivity reactions to local anesthetics. Multiple-dose containers of amide local anesthetics may contain a preservative, methylparaben, the chemical structure of which resembles that of p-aminobenzoic acid. Some patients in whom methylparaben was administered intradermally demonstrate a positive skin reaction (81). Some patients may be allergic to metabisulfite, present in epinephrine-containing local anesthetic solutions. Cross-sensitivity reactions are possible because many other drugs, foods, and beverages contain preservatives such as metabisulfite and hydroxybenzoate. Progressive challenge with dilute (1:1,000) intradermal local anesthetic injections is often obtained to diagnose immunebased adverse responses to local anesthetics. Given the rarity of true, antibody-related, allergic reactions in patients, it is unclear whether skin testing provides cost-effective information for patients who have experienced an apparent allergic reaction. Skin testing by the anesthesiologist may be useful when local anesthetics are needed acutely (82). Clearly, local anesthetic solutions without additives must be used in such testing, and also used for regional anesthesia in patients with a history of allergy to preservatives in foods or drugs (72). Acquired methemoglobinemia: A retrospective series of 138 cases at 2 teaching hospitals. Local Tissue Toxicity that an occasional patient may have a local anesthetic allergy, and both anaphylactic and anaphylactoid responses to local anesthetic are possible (77,78). However, systemic toxic reactions to local anesthetic agents are frequently misdiagnosed as allergic or hypersensitivity reactions (72,79). The ester local anesthetics, especially procaine and benzocaine, have long been assumed to have a greater propensity for allergic reactions based on the fact that they are derivatives of paminobenzoic acid. According to many textbooks, the advent of the amide local anesthetics, none of which is a derivative of para-aminobenzoic acid, appears to have markedly reduced the incidence of allergic reactions to local anesthetic drugs (4). Nevertheless, good data to support this widely (and strongly) held opinion are sparse indeed.
Syndromes
- You have increased thirst or appetite, unexplained weight loss, increased urinary frequency, or fatigue -- these may be signs of diabetes.
- Wound infections
- Fever and chills
- Excessive bleeding
- Cerebral palsy
- Add 1 tablespoon of rice cereal to 2 ounces of formula, milk, or expressed breast milk. If needed, change the nipple size or cut a small x in the nipple.
Neural blockade of oral and circumoral structures can be achieved via extraoral or intraoral techniques arrhythmia list 5 mg plendil order with mastercard. With their in-depth knowledge of intraoral anatomy and familiarity with the oral cavity, most dentists use the intraoral approaches. However, there may be specific indications in which one method is preferred over the other. The presence of anatomic anomalies, infection, the nature of an injury and the extent of the procedure, or the use of local anesthetic techniques for diagnosis or management for acute and/or chronic pain syndromes, for example, may mitigate for or against a particular technique, drug, or approach. Generally, the extraoral approach is designed to provide anesthesia of a major nerve trunk. The effect of this type of blockade is to block neural conduction to a wide area of the face, head, or neck. This article discusses the most common intraoral techniques used by dentists to anesthetize soft and hard tissues of the oral cavity. Local anesthetic techniques involving both intraoral and extraoral approaches to the trigeminal nerve are reviewed. In addition, the armamentarium unique to dentistry and the pharmacology of the local anesthetics routinely employed are presented. Intraoral local anesthesia, as well as dental therapy, is often complicated by the existence of multifactorial psychological considerations associated with the delivery of dental care. Anticipation of pain is the most common cause of anxiety associated with a dental visit and accounts for the avoidance behavior of 6% to 9% of the U. It is imperative for health care professionals to understand and appreciate these issues and employ perioperative behavioral management strategies such as progressive relaxation, hypnosis, biofeedback, systematic desensitization, or the use of sedative drugs to reduce anxiety, fear, and apprehension to acceptable levels. Like any regional anesthetic technique, the effectiveness and utility of any intraoral injection depends upon patient considerations, the extent and duration of the procedure, and the skill and experience of the clinician. Every clinician should be aware of her skill limitations, as well as the limitations of the contemplated technique and agents. These factors must be clearly understood, as they will directly impact on successful outcomes and the potential for severe complications. The management of the apprehensive dental patient remains one of the most challenging problems in health care. Based on this information and practitioner knowledge base, a reasonable and rational anesthesia plan, taking into account the riskbenefit balance, may be successfully formulated. This position offers at least two distinct advantages over the conventional upright or horizontal position. First, the oral cavity can be easily accessed and landmarks identified to provide optimal working conditions for the dentist. Second, this position provides a physiologically sound cardiovascular and respiratory position. Venous return is facilitated from both upper and lower extremities, and diaphragmatic movement is unrestricted. Vasodepressor syncope remains the most common medical emergency in dentistry and is often associated with the administration of local anesthesia. This may be due to the high incidence of phobia and stress or the anticipated (and sometime actual) pain that is often associated with intraoral injections. Tissue Preparation Tissue preparation for regional anesthesia at extraoral sites involves disinfection of the area with a suitable preparatory solutions and the use of appropriate aseptic technique. For local anesthetic injections within the oral cavity, true "asepsis" is neither necessary nor attainable. Nevertheless, certain basic principles may be adhered to , to reduce the risk of infection, particularly into deep structures. Prior to injection, the hands of the operator should be scrupulously cleansed and gloved. A surgical mask and eye protection is worn to protect the operator from inadvertent exposure to blood, saliva, or mucus. Patient should be placed in semi-reclining position with legs and thorax slightly elevated.
Usage: gtt.
Medial and lateral antebrachial cutaneous nerve blocks: An easily learned regional anesthetic for forearm arteriovenous fistula surgery arrhythmia long term effects cheap 2.5 mg plendil with mastercard. Distal nerve blocks at the wrist for outpatient carpal tunnel surgery offer intraoperative cardiovascular stability and reduce discharge time. Nerve blocks at the wrist for carpal tunnel release revisited: the use of sensorynerve and motor-nerve stimulation techniques. Epidural and subarachnoid anesthesia, which provide rapid, reliable, and safe anesthesia of the lower extremities, are more widely taught to anesthesiologists than lower extremity peripheral neural blockade techniques. Unlike the upper extremity, the entire lower extremity cannot be anesthetized with a single injection, and injections are generally deeper than those required for upper extremity block. As early as 1887, Crile performed amputations by exposing the sciatic nerve in the gluteal fold and the femoral nerve in the inguinal fold, and injecting cocaine intraneurally. Braun mentions that blockade of the lateral cutaneous femoral nerve was described by Nystrom in 1909 (2). Laewen expanded on this by describing the additional blockade of the anterior crural nerve, and Keppler improved both techniques by advocating the elicitation of paresthesias. Subsequently, no fewer than six others advocated percutaneous approaches to the sciatic nerve alone. Many of these same authors described blockade of other nerves of the lower extremity as well (Chapter 1). Importantly, many of the techniques currently utilized are nearly identical to the original descriptions. This emphasizes remarks made by Labat that: "Anatomy is the foundation upon which the entire concept of regional anesthesia is built"; and that "The anesthetist should attempt to visualize the anatomic structures traversed by the needle and utilize the tactile senses to determine the impulses transmitted by the point of the needle as it approaches a deep landmark. Labat localized neural structures using fascial "pops" and the elicitation of one or more paresthesias, as well as field infiltration. Advances in needles, catheters, and nerve stimulator technology have facilitated localization of neural structures and improved success rates. The lumbosacral plexus arises from at least eight spinal nerve roots, each of which contains anterior and posterior divisions that innervate the embryologic ventral or dorsal portions of the limb. The nerves to the muscles of the anterior and medial thigh are from the lumbar plexus. The muscles of the buttocks, the posterior muscles in the thigh, and all the muscles below the knee are supplied by the sacral plexus. Although the lumbosacral plexus as a whole contributes to the nerve supply of the lower extremities, the upper part of the lumbar division supplies the iliohypogastric and ilioinguinal nerves, which are in series with the thoracic nerves and innervate the trunk above the level of the extremity (Chapter 16). Specifically, the iliohypogastric nerve provides cutaneous innervation to the skin of the buttock and the muscles of the abdominal wall. The ilioinguinal nerve supplies the skin of the perineum and adjoining portion of the inner thigh (see Chapter 16). A third nerve, the genitofemoral nerve, arises from the first and second lumbar nerves. It also gives off a lumboinguinal branch, which supplies the skin over the area of the femoral artery and femoral triangle (Table 14-1). The branches of the lumbar plexus and the iliohypogastric, ilioinguinal, genitofemoral, lateral femoral cutaneous, femoral, and obturator nerves, emerge from the psoas laterally, medially, and anteriorly. The posterior cutaneous nerve has sometimes been referred to as the "lesser sciatic" nerve. Abbreviations: Sup, superior; Inf, inferior; Lat, lateral; Post, posterior; Cut, cutaneous. Chapter 14: the Lower Extremity: Somatic Blockade 345 L1 - L5 = Lumbar plexus S1 - S4 = Sacral plexus L1 L2 L3 Psoas major m. Inasmuch as the two nerves course through the pelvis together and out through the greater sciatic foramen, they are considered together when techniques for blocking the sciatic nerve above the gluteal fold are discussed. The first is the tibial, derived from the ventral branches of the anterior rami of the fourth and fifth lumbar and first, second, and third sacral nerves. The second is the common peroneal, derived from the dorsal branches of the anterior rami of the same five nerves. These two major nerve trunks pass as the sciatic to the proximal angle of the popliteal fossa, where they separate, with the tibial portion passing medially and the common peroneal (lateral popliteal) laterally.
References
- Bulsiewicz WJ, Kahrilas PJ, Kwiatek MA, et al: Esophageal pressure topography criteria indicative of incomplete bolus clearance: A study using high-resolution impedance manometry. Am J Gastroenterol 104:2721, 2009.
- Waltl B, Melischek M, Schuschnig C, et al: Tracheal intubation and cervical spine excursion: direct laryngoscopy vs. intubating laryngeal mask. Anaesthesia 56:221, 2001.
- Eisert WG. Dipyridamole in antithrombotic treatment. Adv Cardiol 2012;47:78-86.
- Zollo JD, Zeitouni NC: The Roswell Park Cancer Institute experience with extramammary Pagetis disease, Br J Dermatol 142:59n65, 2000.