Ditropan
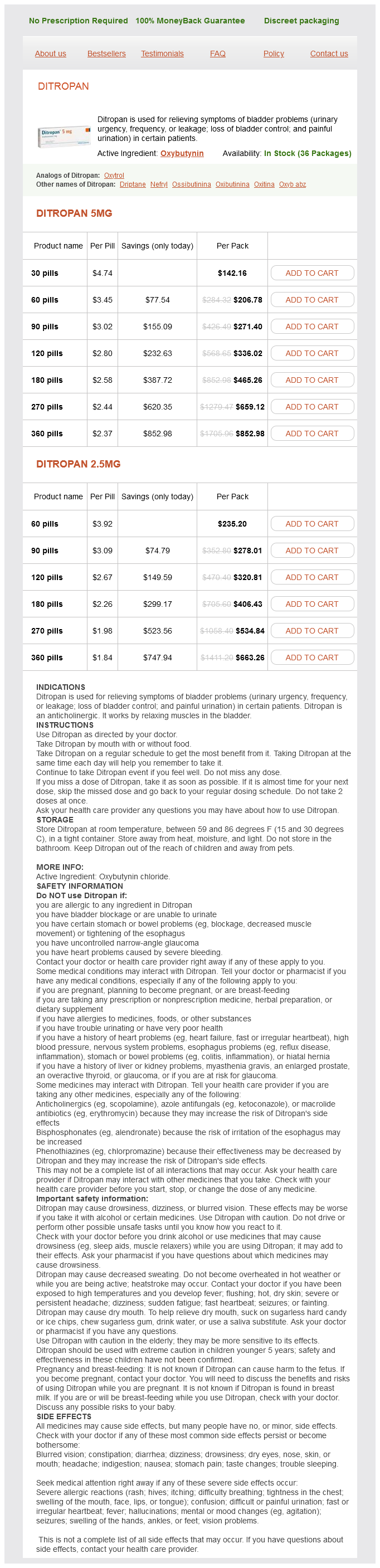
Ditropan 5mg
- 30 pills - $142.16
- 60 pills - $206.78
- 90 pills - $271.40
- 120 pills - $336.02
- 180 pills - $465.26
- 270 pills - $659.12
- 360 pills - $852.98
Ditropan 2.5mg
- 60 pills - $235.20
- 90 pills - $278.01
- 120 pills - $320.81
- 180 pills - $406.43
- 270 pills - $534.84
- 360 pills - $663.26
Clinically gastritis inflammation diet cheap ditropan 2.5 mg buy line, one may test for impaired graphesthesia, or the ability to recognize letters or numbers traced on the skin, or for loss of the ability to tell the direction of a line drawn across the skin. Importantly, some tactile function remains even after complete loss of the dorsal columns, and awareness and localization of nonnoxious tactile stimuli can still occur. Thus at least some of the information carried by the dorsal column pathway is also conveyed by additional ascending pathways. In contrast to the severe deficits in discriminatory touch sensation, cutaneous pain and temperature sensations are unaffected by lesions of the dorsal columns. However, visceral pain is substantially diminished by damage to the dorsal columns. Trigeminal Pathway for Fine-Touch Sensation From the Face Primary afferent fibers that supply the face, teeth, oral and nasal cavities, and cranial meninges synapse in several brainstem nuclei, including the main sensory nucleus and the descending nucleus of the trigeminal nerve. Spinocerebellar and Proprioceptive Pathways Proprioceptors provide information about the positions and movement of parts of the body. In addition to being used for local reflexes (see Chapter 9), this information has two main targets, the cerebellum and the cerebral cortex. The information sent to the cerebral cortex is the basis for conscious awareness of our body parts. These pathways carry both cutaneous and proprioceptive information to the cerebellum. The ventral spinocerebellar tract also provides somatosensory input from the lower limb to the cerebellum. Note the double decussation of the ventral spinocerebellar pathway (one decussation at the spinal cord levels and a second one in the cerebellar white matter). This double crossing highlights the general rule that each half of the cerebellum is functionally related to the ipsilateral side of the body. To provide proprioceptive information from the lower limb to the cerebral cortex, the main axons of the dorsal spinocerebellar tract give off a branch in the medulla that terminates in nucleus z, which is just rostral to the nucleus gracilis. The route to the cerebellum starts with dorsal root ganglion fibers from the cervical spinal levels that ascend in the cuneate fasciculus to the external cuneate nucleus. The axons of the external cuneate nucleus then form the cuneocerebellar tract, which enters the cerebellum via its inferior peduncle. For the head, proprioceptive input is carried by cells of the mesencephalic nucleus of the trigeminal nerve. Recall that the neurons in this nucleus are actually the cell bodies of the primary afferents that innervate stretch receptors in the muscles of mastication (muscles that move the jaw) and in other muscles of the head. The central processes of these neurons project to the trigeminal motor nucleus for local reflexes or to the nearby reticular formation. There are also trigeminocerebellar pathways for conveying somatosensory (tactile and proprioceptive) information from the head to the cerebellum. Thalamic and Cortical Somatosensory Areas Thalamus the ventroposterior nuclear complex of the thalamus represents the main termination site for ascending somatosensory information in the diencephalon. These nuclei also receive input conveying pain and temperature information from the spinothalamic or equivalent trigeminothalamic tracts, respectively. In addition, the spinothalamic tract terminates in parts of the posterior nuclear complex and several other thalamic nuclei. Single-unit recordings from the ventroposterior complex of nuclei have shown that the responses of many of the neurons in these nuclei to stimuli resemble those of first- and second-order neurons in the ascending tracts. The receptive fields of thalamic cells are small but somewhat larger than those of primary afferent fibers. Moreover, the responses may be dominated by a particular type of sensory receptor. The inhibition may actually take place in the dorsal column nuclei or in the dorsal horn of the spinal cord. During a state of drowsiness or during barbiturate anesthesia, thalamic neurons tend to undergo an alternating sequence of excitatory and inhibitory postsynaptic potentials. The alternating bursts of discharges in turn intermittently excite neurons in the cerebral cortex. Such patterns of excitation and inhibition result in an rhythm or in spindling on the electroencephalogram.
Ditropan dosages: 5 mg, 2.5 mgDitropan packs: 30 pills, 60 pills, 90 pills, 120 pills, 180 pills, 270 pills, 360 pills
Through its stimulation of NaCl reabsorption in the collecting duct gastritis jaundice 2.5 mg ditropan buy, aldosterone also indirectly increases water reabsorption by this nephron segment. As noted earlier, aldosterone stimulates both NaCl reabsorption and K+ secretion by the collecting duct. By contrast, during hyperkalemia, K+ excretion by the kidneys is increased to normalize plasma [K+], albeit without an accompanying change in NaCl excretion. This phenomenon-the apparent independent effects of aldosterone on urinary Na+ and K+ excretion-is called the aldosterone paradox. Because the early distal tubule is not directly responsive to aldosterone, this hormone does not stimulate NaCl reabsorption in this segment. Urodilatin is secreted by the distal tubule and collecting duct and is not present in the systemic circulation; thus urodilatin influences only the function of the kidneys. It inhibits NaCl and water reabsorption across the medullary portion of the collecting duct. Uroguanylin and guanylin are produced by neuroendocrine cells in the intestine in response to oral ingestion of NaCl. Studies in Sgk1 knockout mice reveal that this kinase is required for animals to survive severe NaCl restriction and K+ loading. NaCl restriction and K+ loading enhance plasma [aldosterone], which rapidly (in minutes) increases Sgk1 protein expression and phosphorylation. These mutations increase the number of Na+ channels in the apical cell membrane of principal cells and thereby the amount of Na+ reabsorbed. The cause of the autosomal dominant form is an inactivating mutation in the mineralocorticoid receptor. First, NaCl and water reabsorption by the nephron (especially the proximal tubule) falls. Second, aldosterone secretion decreases, thus reducing NaCl reabsorption in the thick ascending limb, distal tubule, and collecting duct. Third, because angiotensin is a potent vasoconstrictor, a reduction in its concentration permits the systemic arterioles to dilate and thereby lower arterial blood pressure. The involvement of these gut-derived hormones helps explain why the natriuretic response of the kidneys to an oral NaCl load is more pronounced than when delivered intravenously. Catecholamines released from the sympathetic nerves (norepinephrine) and the adrenal medulla (epinephrine) stimulate reabsorption of NaCl and water by the proximal tubule, thick ascending limb of the loop of Henle, distal tubule, and collecting duct. Dopamine, a catecholamine, is released from dopaminergic nerves in the kidneys and is also synthesized by cells of the proximal tubule. Adrenomedullin is a 52amino acid peptide hormone that is produced by a variety of organs, including the kidneys. Adrenomedullin induces a marked diuresis and natriuresis, and its secretion is stimulated by congestive heart failure and hypertension. It is the most important hormone that regulates reabsorption of water in the kidneys (see Chapter 35). It increases reabsorption of water by the collecting duct because of the osmotic gradient that exists across the wall of the collecting duct (see Chapter 35). Starling forces regulate reabsorption of NaCl and water across the proximal tubule. Starling forces between this space and the peritubular capillaries facilitate movement of the reabsorbed fluid into the capillaries. Some solute and water reenters the tubule fluid (3), and the remainder enters the interstitial space and then flows into the capillary (2). The width of the arrows is directly proportional to the amount of solute and water moving by pathways 1 to 3. Starling forces across the capillary wall determine the amount of fluid flowing through pathway 2 versus pathway 3. Transport mechanisms in the apical cell membranes determine the amount of solute and water entering the cell (pathway 1). Pi, interstitial hydrostatic pressure; Ppc, peritubular capillary hydrostatic pressure; i, interstitial fluid oncotic pressure; pc, peritubular capillary oncotic pressure. Thin arrows across the capillary wall indicate the direction of water movement in response to each force.
Fermented milk (Kefir). Ditropan.
- Lowering serum cholesterol. Research shows that taking kefir has little or no effect on cholesterol levels.
- What is Kefir?
- How does Kefir work?
- Antibiotic-associated diarrhea. Some research shows that a specific kefir-containing drink (Probugs, Lifeway Foods, Inc.) does not reduce diarrhea caused by antibiotics.
- Dosing considerations for Kefir.
- Other conditions.
- Improving digestion.
- Are there safety concerns?
Source: http://www.rxlist.com/script/main/art.asp?articlekey=97007
Diminished or functionally impaired intraepidermal nerve fibers lead to neuropathic symptoms gastritis symptoms nhs ditropan 2.5 mg buy low cost, including burning and pruritus36. Nerves control vascular tone, as demonstrated in blushing responses, and they mediate the sensations of heat, cold, itch, touch and pain (Chs 5 & 6). Defects in sensation and neurologic function occur commonly, and they may be seen in patients with postherpetic neuralgia, uncontrolled itching, neurologic syndromes. A highly useful therapeutic development has been the intradermal injection of botulinum toxin to uncouple cholinergic nerve fibers. This technique has at least two dermatologic applications: (1) to decrease muscle tone, leading to a loss of facial lines for cosmetic purposes; and (2) to inhibit the excessive sweating that characterizes disabling axillary and palmar hyperhidrosis37 (Ch. Cytokines Abnormality of neurologic communication: excessive sensitivity Itch is a major problem for patients with skin disease (Chs 5 & 6). We presume that modest levels of itching confer some beneficial effect, but, most certainly, excessive itching can be devastating to both personal and social activities. On the other hand, there is at present little evidence for structural abnormalities that predispose to excessive itching. Chief among these cells are dendritic cells, which, after activation, leave the skin and traffic to regional lymph nodes. The processes of activation, outward migration, and repopulation have been areas of intense investigation, with the prospect of developing methods by which immunity may be modulated. Exogenous "sweat" may be created by spraying water over the body repeatedly throughout an exercise or event54. Heat injury as therapy Failure of thermoregulation: effects of excessive cold In contrast to heat injury, individuals exposed to cold temperatures require heating to prevent injury. This also occurs under two related circumstances: (1) in response to heat loss to the environment in amounts that cool the body centrally (hypothermia); and (2) in response to exposure locally to sustained temperatures below freezing, which otherwise would lead to direct freezing injury ("frostbite"). Extreme examples of excessive core and surface cooling in association with limited central heat generation were described vividly by Jon Krakauer in his report of the Mount Everest climbing disasters of 199655. Unfortunately, aside from vascular constriction to reduce radiation of heat from the skin surface and shivering (or exercise) to increase central heating, there are no intrinsic cutaneous mechanisms to protect against excessive cooling. However, humans have become quite adept at creating artificial methods to prevent cold or heat injury through clothing and shelter. Perhaps the most obvious are the mountain climbers who scale the Himalayan mountains and the firefighters who wear insulated clothing as they enter burning buildings. Failure of cytokine and cellular communication Knowledge about the roles of cytokines and cell traffic in cutaneous communication is as yet in its infancy, meaning that defects are only now being recognized. Stemming from an improved understanding of the role of cytokines in keratinocyte biology, major developments in dermatologic therapy have been achieved over the past 15 years in the management of inflammatory skin diseases, most notably psoriasis. As our understanding of cytokine biology increases, new developments in targeted therapy will continue to expand our therapeutic armamentarium. Regulating Temperature: Skin as a Thermoregulatory Organ Regulation of core temperature is a characteristic of all mammals, which, by definition, are euthermic. Because environmental influences tend to change that temperature, there exists an intricate system of regulation in which skin plays a decisive role as both radiator and insulator. Temperature regulation by the skin is effected primarily through evaporative cooling after eccrine sweating (Ch. Human skin includes several million eccrine sweat glands distributed over most of its surface, with the total mass of eccrine glands approximately that of one kidney. Under neurologic control, the secretory activity of eccrine sweat glands consists of two major activities: (1) secretion of an ultrafiltrate of a plasma-like fluid; and (2) reabsorption of sodium by the duct to produce hypotonic sweat. Interpersonal Communication: the Skin Conveys Beauty, Attracts Attention and Contributes to Self-Identity An important function of skin begins with the need for humans to communicate with each other so that personal and societal goals can be met. The skin plays an important role in interpersonal communication by conveying beauty to others, attracting attention, and contributing to the development and expression of self-identity. The presence of beauty, as seen in photographs or paintings, tends to attract attention, which is sometimes intense.
Syndromes
- Creatinine clearance
- Complete blood count (CBC)
- Colonoscopy
- Support groups (such as Alcoholics Anonymous)
- Taking antacids and other heartburn medicines for a long period of time
- Use body-temperature water (cooler or warmer water may cause brief but severe dizziness or vertigo).
- Rash
- Do NOT massage the skin near or on the ulcer. It can cause more skin damage.
- Seizures
Innervation of the Face the arrangement of primary afferent fibers that supply the face is comparable to that of fibers that supply the body and is provided for primarily by fibers of the trigeminal nerve moderate gastritis diet buy 5 mg ditropan fast delivery. Peripheral processes of neurons in the trigeminal ganglion (also called the gasserian or semilunar ganglion) pass through the ophthalmic, maxillary, and mandibular divisions of the trigeminal nerve to innervate dermatome-like regions of the face. The central processes of these neurons terminate in the motor trigeminal nucleus (to subserve segmental reflexes equivalent to the segmental spinal cord reflexes [see Chapter 9]), the reticular formation, and the chief sensory trigeminal nucleus. For example, from the body, fine discriminatory touch information is conveyed by the dorsal columnmedial lemniscus pathway, whereas pain, temperature, and crude touch information is conveyed by the anterolateral system. Proprioceptive information is transmitted by yet another route that partially overlaps with the dorsal columnmedial lemniscal pathway. Note, however, that this functional segregation is not absolute, so, for example, there can be some recovery of discriminative touch ability after a lesion of the dorsal columns. The anterolateral system will be discussed in the section on pain because it is the critical pathway for that information. Here, the central pathways also innervates the teeth, the oral and nasal cavities, and the cranial dura mater. The central processes of trigeminal ganglion cells enter the brainstem at the midpontine level, which also corresponds to the level of the chief sensory trigeminal nucleus (nucleus of cranial nerve V). Some axons terminate in this nucleus (primarily large-caliber axons carrying the information needed for fine discriminative touch), whereas others (intermediate- and small-caliber axons that carry information about touch as well as pain and temperature) form the descending trigeminal tract, which descends through the medulla just lateral to the descending trigeminal nucleus. The dorsal columns are formed by ascending branches of the large myelinated axons of dorsal root ganglion cells (the first-order neurons). These axons enter at each spinal segmental level and travel rostrally up to the caudal medulla to synapse in one of the dorsal column nuclei: the nucleus gracilis, which receives information from the lower part of the body and leg, and the nucleus cuneatus, which receives information from the upper part of the body and arm. Note that across the dorsal columns and across the dorsal column nuclei there is a somatotopic representation of the body, with the legs represented most medially, followed by the trunk and then the upper limb. This somatotopy is a consequence of newly entering afferents being added to the lateral border of the dorsal funiculus as the spinal cord is ascended. Such somatotopic maps are present at all levels in the somatosensory system, at least through the primary sensory cortices. The dorsal column nuclei are located in the medulla and contain the second-order neurons of the pathway for discriminatory touch sensation. These cells respond similarly to the primary afferent fibers that synapse on them (see the earlier description of afferent types). The main differences between the responses of dorsal column neurons and primary afferent neurons are as follows: (1) dorsal column neurons have larger receptive fields because multiple primary afferent fibers synapse on a given dorsal column neuron, (2) dorsal column neurons sometimes respond to more than one class of sensory receptor because of the convergence of several different types of primary afferent fibers on the second-order neurons, and (3) dorsal column neurons often have inhibitory receptive fields that are mediated through local interneurons. The axons of dorsal column nuclear projection neurons exit the nuclei and are referred to as the internal arcuate fibers as they sweep ventrally and then medially to cross the midline at the same medullary level as the nuclei. Knowledge of the level of this decussation is clinically important because damage to the dorsal columnmedial lemniscal pathway below this level, which includes all of the spinal cord, will produce loss of fine somatosensory discriminatory abilities on the same, or ipsilateral, side of the lesion, whereas lesions above this level will produce contralateral deficits. Moreover, because there is a clear somatotopic arrangement of fibers in the medial lemniscus, localized lesions cause selective loss of fine-touch sensations limited to specific body regions. The dorsal columnmedial lemniscus pathway conveys information about fine-touch and vibratory sensations. This information is critical for many of the discriminatory tactile abilities we have. For example, spatial acuity is lowered by damage to this pathway, and the ability to identify objects by their shape and texture can be lost by damage to this pathway. It may also reflect inhibition of the thalamic neurons by recurrent pathways through the reticular nucleus. Thalamic neuron receptive fields are on the side of the body contralateral to the neuron, and the receptive field locations vary systematically across the ventroposterior nuclear complex. Moreover, the fact that thalamic neurons often receive input from only one class of receptor suggests that there are multiple somatotopic maps laid out across the ventroposterior nuclear complex. The spinothalamic tract also projects to other thalamic regions, including the posterior nucleus and the central lateral nucleus of the intralaminar complex of the thalamus. The intralaminar nuclei of the thalamus are not somatotopically organized, and they project diffusely to the cerebral cortex as well as to the basal ganglia (see Chapter 9). The projection of the central lateral nucleus to the S-I cortex may be involved in arousal of this part of the cortex and in selective attention. Somatosensory Cortex Third-order sensory neurons in the thalamus project to the somatosensory cortex. As previously discussed, the S-I cortex, like the somatosensory thalamus, has a somatotopic organization.
Usage: q._h.
Contrasts in Rod and Cone Pathway Functions Rod and cone pathways have several important functional differences in their phototransduction mechanisms and their retinal circuitry gastritis healthy diet buy ditropan 2.5 mg low price. As described previously, rods have more visual pigment and a better signal amplification system than cones do, and there are many more rods than cones. Thus rods function better in dim light (scotopic vision), and loss of rod function results in night blindness. In addition, all rods contain the same visual pigment, so they cannot signal color differences. Furthermore, many rods converge onto individual bipolar cells and the results are very large receptive fields and low spatial resolution. Finally, in bright light, most rhodopsin is bleached, so that rods no longer function under photopic conditions. Cones have a higher threshold to light and thus are not activated in dim light after dark adaptation. They provide high-resolution vision because only a few cones converge onto individual bipolar cells in cone pathways. Moreover, no convergence occurs in the fovea, where the cones make one-to-one connections to bipolar cells. As a result of the reduced convergence, cone pathways have very small receptive fields and can resolve stimuli that originate from sources very close to each other. Photoreceptors (R) synapse on the dendrites of bipolar cells (B) and horizontal cells (H) in the outer plexiformlayer. Loss of cone function results in functional blindness; rod vision is not sufficient for normal visual requirements. Synaptic Interactions and Receptive Field Organization the receptive field of an individual photoreceptor is circular. Light in the receptive field hyperpolarizes the photoreceptor cell and cause it to release less neurotransmitter. The receptive fields of photoreceptors and retinal interneurons determine the receptive fields of the retinal ganglion cells onto which their activity converges. The characteristics of the receptive fields of retinal ganglion cells constitute an important step in visual information processing because all the information about visual events that is conveyed to the brain is contained in ganglion cell activity. Both are described as having a center-surround organization in which the light that strikes the central region of the receptive field either excites or inhibits the cell, whereas the light that strikes a region that surrounds the central portion has the converse effect. The center response of a bipolar cell receptive field is due to only the photoreceptors that directly synapse with the bipolar cell. Photoreceptor cells respond to light with hyperpolarization and a decrease in glutamate release and respond to the removal of light with depolarization and increased glutamate release. This implies that the difference in the center responses of "on" and "off " bipolar cells lies in their response to glutamate. In contrast, on-center bipolar cells have metabotropic glutamate receptors that close their channels in response to glutamate. They are depolarized by light on the center of their receptive field, because the reduced release of glutamate by the photoreceptors results in more open metabotropic channels. Thus on-center bipolar cells are excited by light stimulation of the center of their receptive fields. The antagonistic surround response of bipolar cells is due to photoreceptors that surround those that synapse directly on them. These photoreceptors (which also connect directly with their own bipolar cells) synapse with horizontal cells that participate in complex triadic synapses with many photoreceptors and bipolar cells. The reason for this is that horizontal cells are depolarized by glutamate released from photoreceptors and thus, like "off" bipolar cells, are hyperpolarized in the light. Moreover, because they are electrically coupled to each other by gap junctions, they have very large receptive fields. Thus when darkness surrounds central illumination, there is increased excitation of on-center bipolar cells. Bipolar cells may not respond to large or diffuse areas of illumination, covering both the receptors that are responsible for the center response and those that cause the surround response because of their opposing actions. Thus bipolar cells may not signal changes in the intensity of light that strikes a large area of the retina. On the other hand, a small spot of light moving across the receptive field may sequentially and dramatically alter the activity of the bipolar cell as the light crosses the receptive field from the surround portion to the center and then back again to the surround portion.
References
- Ajmone-Marsan C, Baldwin M. Surgical series in temporal lobe epilepsies. Electrocorticography. In Baldwin M, Bailey P (eds), Temporal Lobe Epilepsy. Springfield, IL: Charles C.Thomas, pp. 368-395, 1958.
- Young NS. Agranulocytosis. In: Young NS, ed. The Bone Marrow Failure Syndromes. Philadelphia, PA: W.B. Saunders; 2000:156-182.
- Gotfredsen K, Wennerberg A, Johansson C, et al. Anchorage of TiO2-blasted, HA-coated, and machined implants: an experimental study with rabbits. J Biomed Mater Res 1995;29:1223- 1231.
- Cordeiro PG, Disa JJ, Hidalgo DA, et al. Reconstruction of the mandible with osseous free flaps: a 10 year experience with 150 consecutive patients. Plast Reconstr Surg 1999; 104:1314-20.
- Chan ED, Morales DV, Welsh CH, McDermott MT, Schwarz MI. Calcium deposition with or without bone formation in the lung. Am J Respir Crit Care Med 2002;165:1654-69.
- Ryder N, Jin F, McNulty AM, et al: Increasing role of herpes simplex virus type 1 in first-episode anogenital herpes in heterosexual women and younger men who have sex with men, 1992n2006, Sex Transm Infect 85(6):416n419, 2009.
- Grau AJ, Brandt T, Buggle F, et al. Association of cervical artery dissection with recent infection. Arch Neurol 1999;56:851.