Citalopram
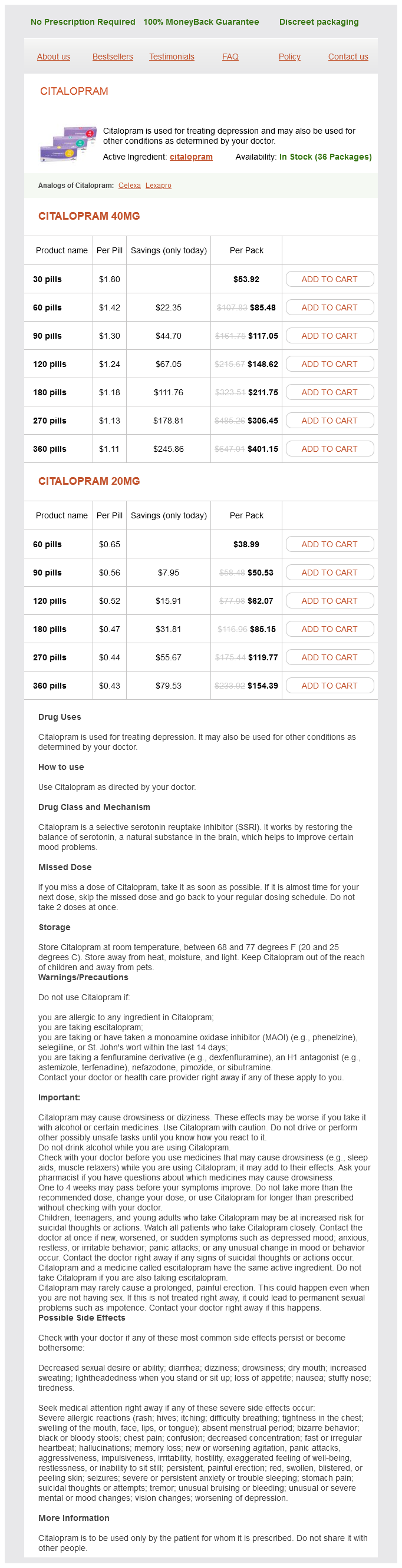
Citalopram 40mg
- 30 pills - $53.92
- 60 pills - $85.48
- 90 pills - $117.05
- 120 pills - $148.62
- 180 pills - $211.75
- 270 pills - $306.45
- 360 pills - $401.15
Citalopram 20mg
- 60 pills - $38.99
- 90 pills - $50.53
- 120 pills - $62.07
- 180 pills - $85.15
- 270 pills - $119.77
- 360 pills - $154.39
Where an absolute maternal indication for delivery is present treatment of lyme disease citalopram 40 mg free shipping, delivery must be effected regardless of gesta tional age or fetal considerations. Management of preeclampsia without severe features Mild preeclampsia is somewhat of a misnomer since it is never a condition to be taken lightly. Disease severity will be determined by symptoms (oedema, epigastric pain, visual disturbance, headache), clinical signs (blood pressure monitoring, hyperreflexia) and investigations. Differentiating mild and moderate disease separately is not necessarily of critical importance as there are no major differences in manage ment through this spectrum of the disease. Women with mild preeclampsia should be managed in hospital or with recurrent pregnancy day assessment admissions where the patient is assessed once or twice weekly for symptoms, clinical features (especially blood pressure) and the above investigations. It is increasingly being replaced by drugs with better side effect profiles such as labetalol and nifedipine. Convulsion prophylaxis Convulsions are potentially lifethreatening to both mother and fetus. Prophylaxis is certainly indicated in the presence of hyperreflexia and some units will use prophylaxis in all cases of severe preeclampsia. Therapy should precede antihypertensive therapy, as magnesium sulfate will have a vasodilatory effect of its own and will also offer some protection against convulsions that may be precipitated by too rapid lowering of the blood pres sure. Anticonvulsant therapy should be continued until at least 12 to 24 hours after delivery. Magnesium sulfate has had a long history of use, and apart from decreasing central nervous system excitability, the vasodilatation induced appears to get at the cause of the problem (focal cerebral ischaemia). A loading dose of magnesium sulfate (4 g = 8 mL of a 50% solution given intravenously over 15 minutes) is followed by a continu ous infusion (1 to 2 g per hour = 2 to 4 mL of a 50% solution). Overdosage may result in serious respiratory depression and can be reversed with intravenous calcium gluconate (10 mL of a 10% solution). Management of severe preeclampsia the presence of severe preeclampsia marks a quantum change in management. Intensive observation and treat ment must be instituted and termination of the preg nancy is required, almost regardless of the period of gestation. At very premature gestations, control of severe hypertension with drugs and/or lesser degrees of protein uria may permit delivery to be deferred temporarily, although frequently the presence of fetal compromise makes delivery indicated anyway. Poorly controlled blood pressure or evidence of other organ damage (renal, hepatic, neurological, haematological, pulmonary) are absolute indications for delivery at any gestational age (Box 16. Blood pressure control Control of severe hypertension is necessary to prevent complications such as cerebral haemorrhage and placental abruption. Nevertheless, rapid and excessive lowering of blood pres sure may aggravate ischaemia in areas of persistent vaso spasm in the brain or placenta. Hydralazine and labetalol are alter natives for intravenous bolus administration to lower blood pressure and can be followed by an infusion. After establishing the diagnosis of severe preeclampsia, the woman should be admitted to an appropriate area of the hospital equipped for intensive nursing. The anaes thetic service should be informed and an obstetric physi cian may be consulted, but the primary responsibility for care must remain with the obstetric team. Intravascular volume status the intravascular compartment is much reduced in severe preeclampsia as a consequence of chronic veno constriction. However, central venous pressure and venous return are maintained for the same reason. Prob lems can occur with the administration of venous compartment dilators (magnesium sulfate and anti hypertensives), which may result in a significant fall in central venous pressure and consequently cardiac output, further compromising tissue perfusion. Practically, the jugular venous pressure and hourly urine output act as barometers of central venous pressure. If fluid replacement Stabilisation prior to delivery A number of principles of management for stabilisation of the disease prior to delivery need to be followed accord ing to an established hospital protocol for the condition. Ergometrine is contraindicated for the third stage and oxytocin (5 units intravenously) should be used instead. The puerperium After delivery, the pathophysiological abnormalities are reversed fairly rapidly; for example, the low renal perfusion/output and depressed platelet levels usually return to normal in 3 to 4 days. If the disorder is severe and has occurred in the second or early third trimester, recurrence is likely in the succeeding pregnancy. Haematology, liver and renal function Transfusion of platelets and/or fresh frozen plasma/ plasma concentrates may be required as judged by hae matological studies.
Citalopram dosages: 40 mg, 20 mgCitalopram packs: 30 pills, 60 pills, 90 pills, 120 pills, 180 pills, 270 pills, 360 pills
Only with this information should the sex of rearing be determined and a name given to the newborn medications j-tube purchase citalopram 20 mg mastercard. Treatment is by careful attention to feeding and then surgical correction of the lip in the first few months. The risk is related very much to maternal age, ranging from about 1 in 2000 at age 18 years to 1 in 40 at age 45 years. The cause in 95% of cases of trisomy 21 is non-disjunction during oogenesis in the mother. About 30% of all babies with Down syndrome are born to mothers over the age of 35 years. About 70% of women of this age group choose to have screening by amniocentesis or chorionic villus sampling followed by termination of the affected fetus. The clinical diagnosis is often suspected because of the presence of a number of characteristic features in the newborn. Limbs: short, broad hands and short, incurved little fingers with single phalangeal crease, bilateral single palmar creases, wide spacing between first and second toes. Neurodevelopmental: generalised hypotonia is very common (> 75%) and there may be associated difficulty with feeding; mild to moderate intellectual impairment is usual. Cardiovascular: congenital heart defects, most commonly atrial and ventricular septal defects, occur in 40%. A Characteristic facial features with upward-slanting palpebra fissures, epicanthal folds, and flat nasal bridge. Sexchromosomeabnormalities Many sex chromosome abnormalities are not associated with phenotypic differences in the newborn period and are usually not diagnosed until later. As such, the same questions may be asked repeatedly, and need to be answered repeatedly and calmly. There should be adequate opportunity for the parents to obtain further information and to be supported through this period. Information written in language that is appropriate for a lay person may be useful. A realistic appraisal of the prognosis should be discussed frankly with the parents. Here the issue of interest is the particular risk that a child may be affected by the condition and the implications for such a child. If conception has occurred, the issue of interest is whether a diagnosis can be made on the fetus. This may involve ultrasound imaging, or molecular genetic or histochemical tests on fetal tissue. This is a rapidly advancing area and gene sequences coding for particular diseases are being discovered regularly. Maternal antibodies can be protective or potentially destructive: they can cross the placenta and provide passive immunity or cause haemolysis or thrombocytopenia. Anaemia in a newborn may occur as the result of haemolysis, infection or blood loss. Polycythaemia (haematocrit > 65%) occurs in response to chronic fetal hypoxia and/or is seen in newborns who are small for gestational age. Haemorrhagic disease of the newborn can be almost completely eradicated by the routine administration of vitamin K to the newborn in the immediate postnatal period. By term, unless there is a reason for increased haemopoiesis, all red cell production is in the bones. In the second and third trimesters, over 90% of haemoglobin is haemoglobin F (Hb F or 22), which is structurally different from adult haemoglobin, haemoglobin A (Hb A 22). There are two compensatory mechanisms which allow adequate oxygen transport in the fetus despite normal fetal PaO2 being 25 mmHg. First, Hb F binds oxygen more avidly than Hb A and can therefore bind more oxygen at a given partial pressure of oxygen. Second, the relatively hypoxic environment of the fetus causes an increase in red cell production and hence the fetus has a higher haemoglobin concentration than later in life. At delivery, with the marked increase in PaO2 which occurs with lung respiration, erythropoietin production in the kidney is suppressed and red cell production is reduced. Haemoglobin decreases to a mean of 14 g/dL at 1 month of age and reaches a nadir at 3 months of age when the mean value is 11 g/dL. This stimulates erythropoietin production and the haemoglobin subsequently increases to adult levels.
Geum (Avens). Citalopram.
- What is Avens?
- Dosing considerations for Avens.
- Diarrhea, colitis, uterine bleeding, fevers, and other conditions.
- How does Avens work?
- Are there safety concerns?
Source: http://www.rxlist.com/script/main/art.asp?articlekey=96324
Fetal infection is particularly uncommon when the maternal infection occurs after the 20th week of gestation symptoms zoloft dose too high 40 mg citalopram purchase with amex. Presentation in the newborn can be similar to congenital toxoplasmosis or cytomegalovirus, although with particular propensity for growth restriction, cataracts, congenital heart disease, deafness and bone lesions. Specific diseases, and treatments where available, are discussed throughout the chapter. With severe involvement, the common features are microcephaly, intracranial calcification, neurological impairment. Newborn infection can still occur even when there is no history of active vaginal herpetic lesions at the time of delivery. If the maternal herpes infection is primary, there will be no passive immunity and neonatal infection is more likely. The infection can present in the first week either as a serious, non-specific, septic-like illness or with a cutaneous vesicular rash. Diagnosis is by culture of the herpes virus from cerebrospinal fluid, or from samples taken from the eye, nose, throat, urine or faeces. Despite an improvement in prognosis with aciclovir, there is still Chapter 72 Neonatal Infection an appreciable mortality rate and neurological morbidity in survivors. The management of delivery in the presence of known active vaginal infection is discussed in previous chapters. For example, six cases were reported (via mandatory notification) in Western Australia from 1991 to 2009. Asymptomatic infection of the newborn may develop signs of the disease months or even years later. When mucocutaneous syphilitic lesions are found in the newborn, there may be associated anaemia, oedema, failure to thrive, pyrexia and osteochondritis. Adding to this are difficulties in interpreting serological diagnostic tests: positive serology may indicate a previous maternal infection and the absence of seropositivity does not necessarily exclude the diagnosis. Hence, clinical or radiographic signs of syphilis, especially if the mother had a history of syphilis during the pregnancy, warrant initiation of treatment. In neonates, treatment with a single dose of benzathine penicillin (50 000 units/kg) intramuscularly may suffice. Alternatively, 10-day treatment regimes also exist: benzylpenicillin 50 mg/kg intravenously every 12 hours. Infant scales, baths and other communal areas should be wiped with antibacterial solution and scales covered with a clean towel or paper for each weighing. Perinatally acquired neonatal infections can be acquired in utero, during the birthing process or in the immediate postnatal period. Systemic infection: neonatal bacterial sepsis and nosocomial-acquired infections in neonatal intensive care units. Thrush (candidiasis) Candida albicans is the fungus that causes oral and cutaneous thrush. In the mouth, the lesions present as thick, white, raised plaques with surrounding erythema. Cutaneous candidal infection in the nappy area presents as an erythematous rash with a clearly demarcated border. Treatment is with miconazole or nystatin preparations, either orally or topically depending on the site of infection. In this case it may be in the sick preterm, where invasive catheters and antibiotic use predispose them to fungal infection. The incidence of transmission (and hence infection) during this period can be minimised by attention to the following procedures. Handwashing is the most important method to prevent the transmission of perinatally acquired infections. Adequate handwashing with an antibacterial solution, or the use of antibacterial gel, is necessary before examination of any newborn.
Syndromes
- Redness and tenderness around the ulcer
- Morquio syndrome
- Academy for Eating Disorders - www.aedweb.org
- Most people do not need to take antibiotics every day to prevent diarrhea while traveling.
- Problems with coordination
- Tricyclic antidepressants such as protriptyline or imipramine
Prediction of which pregnancies are at risk is paramount in the organisation of in utero transfer symptoms 0f brain tumor generic 40 mg citalopram visa. Transfer of the mother undelivered is safest for the high-risk fetus that is likely to need neonatal intensive care. An ability to stabilise the unexpectedly sick newborn prior to retrieval is required. Level 2 provides more sophisticated care, including intravenous fluids and basic respiratory support. Postnatal retrieval refers to the transfer of a newborn who is in need of a higher level of newborn care. As such, the newborn is ideally retrieved from the hospital of birth by a fully equipped retrieval service. Every effort must be made to deliver the high-risk newborn at the site where the necessary level of newborn care is available. Transfer of the fetus in utero is preferable, because delivery in a peripheral hospital and subsequent retrieval is associated Source: Courtesy of Prof. In some cases, the need for newborn intensive care has not been anticipated: preterm delivery may have occurred in an apparently low-risk mother or a complication such as antepartum haemorrhage necessitated preterm delivery. If this occurs in a level 1 or level 2 setting, these newborns will require transport by a retrieval team to a more appropriate tertiary unit. Ideally, the nearest regional level 3 newborn unit provides a retrieval facility, which comprises a constantly manned telephone advice line and a mobile intensive care cot. The mobile cot is manned by staff with current skills in newborn intensive care who are also conversant with the particular issues involved in retrieval, such as pressure differences that occur with altitude in aircraft retrievals. These guidelines may vary depending on the availability of local facilities and expertise. Just under one-quarter of neonates in level 3 nurseries around Australia and New Zealand have been retrieved from a lower level nursery setting. Altitude (helicopter or fixed-wing plane transport) reduces the ambient oxygen pressure and needs to be taken into consideration. They should have an opportunity to meet the retrieval team and farewell their baby. If the mother is not to be transferred immediately, every effort should be made to allow motherÂbaby interaction (albeit briefly) prior to transport. Information about the retrieval team and the hospital where the newborn will be cared for should be left with the immediate family. Clinical decisions will be made on the need for cannulas, chest drains or endotracheal intubation for assisted ventilation. These should be made if necessary prior to moving the newborn; procedures may be difficult and hazardous during transport. Monitoring of vital signs (heart rate, oxygen saturation, temperature), blood sugar and blood gases should be undertaken. The mother should be transferred either with the newborn or as soon as possible afterwards. It is desirable that she be with her baby, so that expressed breastmilk is available for her baby when required and that maternal infant bonding is promoted. Even in the case of maternal separation, expressing of colostrum/breastmilk can continue with midwifery support. Prematurity 32 weeks Respiratory distress requiring > 40% oxygen Severe birth asphyxia Convulsions Recurrent apnoea Jaundice requiring exchange transfusion Severe or multiple abnormalities requiring diagnosis or management Need for surgery Suspicion of severe cardiac disease Source: Courtesy of Prof. The transport system must be equipped and staffed so that it becomes an extension of an intensive care nursery. Before the delivery of a preterm newborn, many issues will be of concern to the parents. Hence, they will receive some reassurance in having expectations regarding the following issues discussed: birth weight and physical appearance risk of death and serious morbidity duration of hospitalisation procedures (resuscitation, intubation, ventilation, surfactant) diseases (respiratory distress syndrome, sepsis, jaundice) need for transport to a tertiary centre (if the baby is not born there) the role of parents in intensive care. Thankfully, as discussed in this chapter, there are generally good long-term survival outcomes and an overall low risk of significant disability.
Usage: q.i.d.
Because congenital cardiac anomalies are found in 1/2 of the patients symptoms to diagnosis generic citalopram 40 mg fast delivery, all patients with this syndrome should have cardiac evaluation and close follow-up. Various criteria exist for what is considered normal erectile activity at night, but normal is usually 4Â5 erectile episodes per night with a mean duration >30 min and an increase in circumference of >3 cm at the base and >2 cm at the tip, as well as maximal rigidity above 70% at both base and tip. Validated nomograms have been developed for all major urologic cancers, as well as for some benign urologic diseases. Several studies suggest its utility as a marker for bone turnover in osteoporosis, and for response to treatment of bony metastasis and bisphosphonate therapy. Nocturnal monitoring devices measure the number of erectile episodes, maximal penile rigidity, tumescence, and duration of erections. This testing assumes that the mechanism for nocturnal erections is the same as that for erotically induced erections. Are consecutive nightly recordings required for valid evaluation of sleep-associated erections? Presentation classically is due to gross hematuria caused by left renal vein hypertension. Various modalities, including nephrectomy, autotransplantation, renocaval reimplantation, and venolysis have been employed. Gore-Tex graft renal vein interposition and anterior nephropexy have been successful (Image). Diagnosis and surgical treatment of nutcracker syndrome: A single-center experience. Cardiovascular comorbidities of obesity have been well established and there is mounting evidence that obesity impacts a number of urologic diseases. Prostate cancer has been shown to be more prevalent in obese patients as is adverse pathology. The increased incidence in prostate cancer in obese men is postulated to result, at least partially, by conversion of testosterone to estradiol in adipocytes. Likewise, this aromatization of androgens leads to decreased fertility in young males. Sexual dysfunction is observed in obese men as a result of increased rates of hypertension, diabetes, and vascular disease. Severe oligospermia occurs if counts are <10 million/mL, and may be due to hormone deficiency. A count of <20 million/mL is associated with substantially decreased fertility rates. Surgeons must be aware of this response so as not to cause inadvertent injury, such as perforation of the bladder. Oligozoospermia, azoospermia, and other semen-analysis terminology: the need for better science. Exstrophy of the cloaca includes the persistence and exstrophy of a common cloaca that receives ureters, ileum, and a rudimentary hindgut and is associated with failure of fusion of the genital tubercles and pubic rami. Other anomalies include incomplete development of the lumbosacral vertebrae with spinal dysraphism; imperforate anus; cryptorchidism and epispadias in males; anomalies of the mullerian duct derivatives in Ð females; and a wide range of urinary tract anomalies including renal defects. Omphalocele (a defect in the umbilical ring, through which the peritoneum and an amnion-covered sac herniate) is common, and most patients have a single umbilical artery. The questionnaire can be administered without the supervision of a professional interviewer. It focuses on the symptoms of urinary urgency, frequency, nocturia, and dysuria/ pain over a 30-day period. It has been found useful as a tool to follow symptoms of but not the diagnosis of interstitial cystitis. In addition, excessive hip flexion or cautery injury during surgery can cause neurapraxia of the obturator nerve. The incidence of intraoperative obturator nerve injury is not well documented but thought to be rare. When transection of the obturator nerve is identified intraoperatively, surgical repair may be done by end-to-end anastomosis or grafting when achieving tension-free anastomosis is not possible. Nerve transection can be repaired with end-to-end approximation of nerve edges with four 6Â0 to 10Ânylon or Prolene epineural stitches, using magnification if possible. If the nerve is frayed and grossly devitalized, efforts can be made to trim both segments sharply.
References
- Barris RW, Schuman HR. Bilateral anterior cingulate gyrus lesions. Syndrome of the anterior cingulate gyri. Neurology 1953;3:44.
- Hadley JM, Ridley N, Djazaeri B, Glover G. The radiological appearances after endoscopic cricopharyngeal myotomy: Dohlman's procedure. Clin Radiol. 1997; 52:613-615.
- Price RF, Sellar R, Leung C, et al. Traumatic vertebral arterial dissection and vertebrobasilar arterial thrombosis successfully treated with endovascular thrombolysis and stenting. Am J Neuroradiology 1998;19:1677.
- Granowitz EV, Brown RB. Antibiotic adverse reactions and drug interactions. Crit Care Clin. 2008;24:421-442.
- Fujii S, Fukui A, Fukushi Y, et al. The effects of clomiphene citrate on normally ovulatory women. Fertil Steril 1997; 68:997-999.
- Hollander W. Role of hypertension in atherosclerosis and cardiovascular disease. Am J Cardiol 1976; 38:786.
- Burns TM, Bauermann ML. The evaluation of polyneuropathies. Neurology. 2011;76:S6-S13.
- Petzelbauer P, Zacharowski PA, Miyazaki Y, et al: The fibrin-derived peptide Bbeta15- 42 protects the myocardium against ischemia-reperfusion injury. Nat Med 2005;11: 298-304.