Celexa
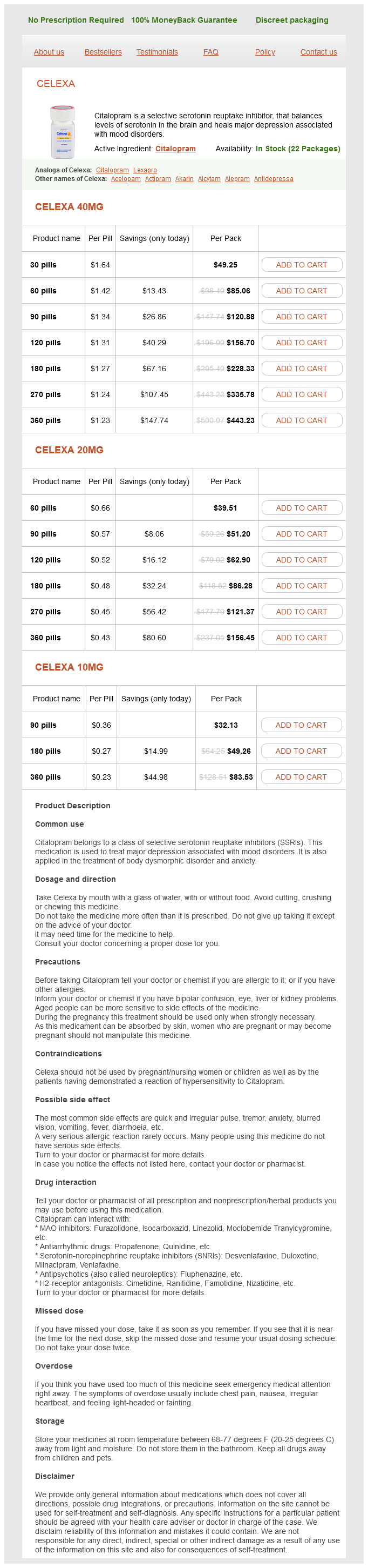
Celexa 40mg
- 30 pills - $49.25
- 60 pills - $85.06
- 90 pills - $120.88
- 120 pills - $156.70
- 180 pills - $228.33
- 270 pills - $335.78
- 360 pills - $443.23
Celexa 20mg
- 60 pills - $39.51
- 90 pills - $51.20
- 120 pills - $62.90
- 180 pills - $86.28
- 270 pills - $121.37
- 360 pills - $156.45
Celexa 10mg
- 90 pills - $32.13
- 180 pills - $49.26
- 360 pills - $83.53
Gene expression profiling of the tumor microenvironment during breast cancer progression medicine z pack celexa 20 mg buy without a prescription. Genomic and mutational profiling of ductal carcinomas in situ and matched adjacent invasive breast cancers reveals intra-tumor genetic heterogeneity and clonal selection. Replication behaviour of heterochromatin as observed by premature chromosome condensation. Mutational evolution in a lobular breast tumor profiled at single nucleotide resolution. Phenotypic and functional characterization in vitro of a multipotent epithelial cell present in the normal adult human breast. Cancer stem cells in solid tumors: accumulating evidence and unresolved questions. The clonal and mutational evolution spectrum of primary triple-negative breast cancers. Transcriptome analysis of the normal human mammary cell commitment and differentiation process. How Darwinian models inform therapeutic failure initiated by clonal heterogeneity in cancer medicine. The most widely used classification of invasive breast cancers, and that used in this chapter (with minor modifications), is that of the World Health Organization (1). This classification scheme is based on the growth pattern and cytologic features of the invasive tumor cells and does not imply histogenesis or site of origin within the mammary duct system. For example, although the classification system recognizes invasive carcinomas designated "ductal" and "lobular," this is not meant to indicate that the former originates in extralobular ducts and the latter in lobules. In fact, subgross whole organ sectioning has demonstrated that most invasive breast cancers arise in the terminal duct lobular unit, regardless of histologic type (2). The most common histologic type of invasive breast cancer by far is invasive (infiltrating) ductal carcinoma. In fact, the diagnosis of invasive ductal carcinoma is a diagnosis by default, since this tumor type is defined as a type of cancer not classified into any of the other categories of invasive mammary carcinoma (1). In this chapter, the terms invasive ductal carcinoma, infiltrating ductal carcinoma, and infiltrating or invasive carcinoma of no special type are used interchangeably. The distribution of histologic types of invasive breast cancer has varied among published series (Table 25-1). These differences may be related to a number of factors including the nature of the patient population and variability in the confines of definition for the different histological types. In general, special type cancers comprise approximately 20% to 30% of invasive carcinomas, and at least 90% of a tumor should demonstrate the defining histological characteristics of a special type cancer to be designated as that histological type (6). The widespread use of screening mammography has had a dramatic impact on the nature of invasive breast cancers encountered in clinical practice. The value of mammography in detecting more cases of ductal carcinoma in situ, smaller invasive breast cancers, and fewer cancers with axillary lymph node involvement is well recognized. However, mammography has also resulted in a change in the distribution of the histological features of the invasive breast cancers detected. In particular, special type cancers (particularly tubular carcinomas) and cancers of lower histological grade are more frequently observed in mammographically screened populations than in patients who present with a palpable mass, particularly in the prevalent round of screening. Most invasive breast cancers have an associated component of in situ carcinoma, although the extent of the in situ component varies considerably. The prevailing view has long been that the invasive carcinomas derive from the in situ component. This is based not only on the frequent coexistence of the two lesions, but on the histological similarities between the invasive and in situ components within the same lesion. In addition, studies evaluating profiles of biological markers and genetic abnormalities have shown that coexisting invasive and in situ carcinomas often share the same immunophenotype and genetic alterations. The routine pathologic examination of invasive breast cancers has extended beyond simply determining and reporting the histologic type of the tumor. Although histologic typing provides important prognostic information in and of itself, other morphologic features that are evaluable on routine histologic sections are also of prognostic value. In this chapter, the various histologic types of invasive breast cancer will be discussed as will pathologic features important in the assessment of prognosis (prognostic factors) and response to therapy (predictive factors).
Celexa dosages: 40 mg, 20 mg, 10 mgCelexa packs: 30 pills, 60 pills, 90 pills, 120 pills, 180 pills, 270 pills, 360 pills
This nomogram is not used at Memorial Sloan-Kettering Cancer Center to determine the need for axillary dissection nor the need for axillary irradiation treatment 7th march celexa 40 mg purchase line. At a median follow-up of 13 months (range, 129 months), no axillary recurrences have occurred in this patient cohort, but longer follow-up is needed. At this time, it is uncertain whether or not additional fields are needed to treat the full axilla in patients estimated to have a high risk of positive non-sentinel nodes. If a decision is made to add additional fields, the full axilla should be treated. Morbidity of Whole Breast Irradiation Treatments require only 15 to 30 minutes each day, and most patients can continue their daily routines with minimal interruptions. Two short-term complications that occur in the majority of patients are fatigue and mild breast dermatitis. The degree of fatigue varies a great deal among individuals and generally improves to baseline within a month after treatment. The skin reactions associated with radiation delivered with modern techniques are typically mild. Erythema, warmth, mild discomfort, and pruritis typically develop toward the end of treatment and improve shortly after treatment completion. Modern treatments are very safe, with a very low likelihood of a permanent normal tissue injury. However, most series report that 80% to 95% of patients have good to excellent aesthetic outcomes after breast irradiation to total doses of 45. The development of a second cancer induced by radiation treatments of the breast is a very unusual event. In an analysis based on the Connecticut cancer registry database of 41,109 breast cancer patients, Boice et al. Given these data, it is important to optimize techniques to minimize scatter radiation dose to the contralateral breast. The newer modulated techniques that provide three-dimensional dose compensation with multileaf collimated subfields have the additional benefit of decreasing the dose to the contralateral breast by 65% to 82% (91). Smoking is recognized as an important cofactor for the development of lung cancer after breast cancer radiation treatments. A rare, but frequently fatal, radiation-related malignancy is lymphangiosarcoma of the treated skin. This is an unusual second cancer in that it can be seen prior to 5 years post treatment. One of the most significant potential sequelae of whole breast irradiation is cardiovascular disease with associated cardiac-related death. This result was predominantly seen in relatively older postmastectomy radiation studies that utilized treatment techniques and dose schedules no longer in use. With the advent of improved technologies, radiation treatments are much less likely to cause adverse cardiac events. Additionally, investigators from Duke University have shown that inclusion of some of the left ventricle in tangential fields used to treat left-sided breast cancers can result in cardiac perfusion abnormalities (98). The period from treatment to radiation-induced cardiac disease is protracted and typically greater than 10 to 15 years, so avoiding direct cardiac exposure is particularly important in younger patients. Based on these data, it is very important that the risk of radiation-associated heart disease be minimized or completely avoided by ensuring that the heart is not within the treatment fields. For patients with upper outer quadrant tumors, a small heart block can be used, which shields a small volume of the far medial and far lateral lower breast tissue. Studies have reported that use of heart blocks do not increase the risk of in-breast recurrence (99). For tumors in the lower quadrants, new techniques are available to physically displace the heart from the tumor bed through breath-hold techniques. As seen on the fused axial (A) coronal (B) image of a free-breathing scan and a breath-hold scan, deep inspiration lowers the diaphragm and displaces the heart inferomedially. The next two axial images show the relationship of the heart to the radiation fields under free-breathing conditions (C) and breath-hold conditions (D). In this example, the treatment beam is only turned on during breath-hold periods to ensure that the heart is outside of the field. In this procedure, patients can monitor their respiratory cycle and hold their breath in a predefined volume that achieves cardiac displacement.
Burdock. Celexa.
- Are there safety concerns?
- What is Burdock?
- Are there any interactions with medications?
- How does Burdock work?
- Fluid retention, fever, anorexia, stomach conditions, gout, acne, severely dry skin, and psoriasis.
- Dosing considerations for Burdock.
Source: http://www.rxlist.com/script/main/art.asp?articlekey=96153
Prevention of breast cancer in the rat with 9-cis-retinoic acid as a single agent and in combination with tamoxifen symptoms zika virus celexa 20 mg order without prescription. Prevention of second primary tumors with isotretinoin in squamous-cell carcinoma of the head and neck. Metformin and incident breast cancer among diabetic women: a population-based case-control study in Denmark. Metformin and pathologic complete responses to neoadjuvant chemotherapy in diabetic patients with breast cancer. Metformin in early breast cancer: a prospective window of opportunity neoadjuvant study. Effect of statins combined with estradiol on the proliferation of human receptor-positive and receptornegative breast cancer cells. Estrogen receptor-negative breast cancer is less likely to arise among lipophilic statin users. Fluvastatin reduces proliferation and increases apoptosis in women with high grade breast cancer. A short-term biomarker modulation study of simvastatin in women at increased risk of a new breast cancer. Statin prescriptions and breast cancer recurrence risk: a Danish nationwide prospective cohort study. Cancer prevention and treatment using combination therapy with plant- and animal-derived compounds. Prevention of tumorigenesis in p53-null mammary epithelium by rexinoid bexarotene, tyrosine kinase inhibitor gefitinib, and celecoxib. Colorectal cancer risk, chronic illnesses, operations, and medications: case control results from the Melbourne Colorectal Cancer Study. A randomised, double blind, placebo controlled study of celecoxib, a selective cyclooxygenase 2 inhibitor, on duodenal polyposis in familial adenomatous polyposis. Aspirin and non-steroidal anti-inflammatory drugs for cancer prevention: an international consensus statement. Effect of daily aspirin on longterm risk of death due to cancer: analysis of individual patient data from randomised trials. Chemoprevention of breast cancer in rats by celecoxib, a cyclooxygenase 2 inhibitor. Risk of acute myocardial infarction and sudden cardiac death in patients treated with cyclo-oxygenase 2 selective and non-selective non-steroidal anti-inflammatory drugs: nested casecontrol study. Rofecoxib and cardiovascular adverse events in adjuvant treatment of colorectal cancer. Duration of treatment with nonsteroidal anti-inflammatory drugs and impact on risk of death and recurrent myocardial infarction in patients with prior myocardial infarction: a nationwide cohort study. Diabetes, metabolic syndrome, and breast cancer: a review of the current evidence. Progesterone stimulates mammary gland ductal morphogenesis by synergizing with and enhancing insulinlike growth factor-I action. It consists of a grape-like aggregate of acini surrounded by specialized mammary stroma. The acini drain into a terminal ductule, part of which is intralobular, and part extralobular. The luminal epithelium lining the glandular lumen has a polarized morphology, with the nucleus at one pole of the cell and an apical cytoplasmic compartment at the other end. Estrogen and progesterone play a central role in regulating the growth and differentiation of normal breast tissue. Whether all breast epithelium has the potential to transform or this capability is limited to epithelial stem cells or progenitor cells is a topic of research and debate. Few authors have documented silent chromosomal alterations in morphologically normal epithelial cells, and suggested that they may predispose to premalignant or malignant transformation (2).
Syndromes
- Gums (gingiva)
- Trouble breathing
- High blood pressure
- Lacks moral concepts of right and wrong
- Ear pain
- Pulmonary valve stenosis
- Bulging fontanelles in infants
- Infection
- Infection
- Sigmoidoscopy
Therefore treatment regimen purchase generic celexa, confining radiation to the area immediately surrounding the tumor may provide equivalent rates of primary tumor control while sparing radiation to regions that are at low risk of harboring clinically relevant microscopic disease. Accordingly, there has been an interest in studying whether the treatment course can be shortened without compromising the efficacy or increasing the toxicity of the therapy. Because less total tissue is irradiated, higher daily doses can be delivered over fewer fractions, making treatment more convenient for patients. Although the modalities vary significantly, all are designed to deliver therapeutic doses to the tissue near the surgical cavity that is felt to be at highest risk of recurrence. These techniques have the advantage of being noninvasive and can utilize many of the same treatment planning and delivery tools as whole breast irradiation. No clear dose-toxicity relationship has been identified-although initial results are promising- but long-term follow-up is lacking (79). The number and position of catheters is determined by the size and shape of the surgical cavity. Once inserted, the catheters are after-loaded at predetermined locations in order to deliver the target dose to the breast tissue immediately surrounding the surgical cavity. Due to the steep dose falloff, interstitial brachytherapy allows for rapid delivery of high radiation doses to target tissues with nearly complete sparing of surrounding normal structures. However, due to the invasive nature of the procedure, infection, fat necrosis, or scarring can occur. Several interstitial brachytherapy experiences for earlystage breast cancer have been published. The 5-year rate of fat necrosis in these patients was 11%, but 95% to 99% of cosmetic outcomes were reported as good to excellent. While in retrospect, the technique of interstitial implant in this trial was not ideal, the results illustrate the need for very long follow-up to adequately assess both local tumor control and toxicity with unconventional fractionation. The device is inserted into the lumpectomy cavity during surgery or several days following surgery (after pathologic confirmation of margin status) and inflated. Alternate devices with multiple lumens are also available and allow for greater flexibility in treatment planning. Advantages of intracavitary brachytherapy include its ease of use compared to interstitial techniques and its reproducibility in delivery of radiation dose to the balloon surface. However, problems with dose homogeneity can occur when the surgical cavity is irregularly shaped, and treatment of superficial cavities can lead to a high skin dose and increased toxicity. Two-year data from a multi-institutional series of 483 patients treated using the MammoSite applicator show a 1. The technique has been criticized for not delivering adequate dose to a sufficient margin around the cavity. Another disadvantage of intraoperative radiation is that pathologic information regarding margin status and lymph node involvement are not available at the time of treatment. If unfavorable pathologic features are found, subsequent whole breast irradiation can be administered. The results of the trial suggest superior local control with whole breast irradiation, but several factors limit its applicability. Microscopic margin status was not evaluated in these patients, and axillary lymph node staging was not performed. The doses used for whole breast irradiation are significantly lower than typically used today, and no boost was given. Many patients had poor prognostic factors, including large tumor size, non-ductal histology, high grade, and the presence of lymphovascular invasion that today would prompt more aggressive therapy. Once again, the lack of microscopic margin status severely limits the findings of this trial. The trial is limited by the relatively small number of patients, short follow-up, and variability in treatment within each arm across institutions. The number of patients with major toxicity was similar between arms; however, the type of complications varied. There is ongoing debate about whether more groups of patients should be considered suitable. A 2011 analysis of Medicare data suggests that the use of brachytherapy following breast-conserving surgery has increased from <1% of new breast cancer cases in 2001 to 10% of cases in 2006. Although many of these trials are accruing briskly and early toxicity results may be available in the next several years, many more years will be required before data regarding long-term efficacy and safety are available.
Usage: q.h.
Changes in circulating estrogen levels can induce abnormalities of the central thermoregulatory centers medicine in balance 10 mg celexa otc, resulting in hot flashes. Perspiration and vasodilation, classic mechanisms of heat loss controlled by the hypothalamus, are activated during a hot flash. In normal homeostasis, these mechanisms are activated to maintain core body temperature in a regulated range termed the "thermoregulatory zone. In women undergoing natural menopause there is an association of hot flash symptoms with maternal history of hot flashes and with cigarette smoking. For these reasons, many women assume that hot flashes are an inevitable symptom of being a breast cancer survivor. In breast cancer patients, vasomotor symptoms negatively impact sleep, quality of life, energy, as well as compliance with therapy and satisfaction with treatment decisions. The cause of vasomotor symptoms in breast cancer patients can be the result of abrupt estrogen loss due to surgery or chemotherapy, the use of adjuvant hormonal therapy, discontinuation of hormone replacement therapy, or from natural menopause. Tamoxifen, the most commonly prescribed pharmacologic treatment for breast cancer over the past decade, is associated with hot flashes in more than 50% of users (3,4). Tamoxifen-associated hot flashes increase over the first several months of treatment and then gradually resolve (3). Postmenopausal women with a history of significant hot flashes prior to tamoxifen and a history of prior estrogen therapy use are likely to experience more severe hot flashes with tamoxifen therapy (3,5). In premenopausal women with breast cancer, adjuvant chemotherapy is frequently associated with temporary or permanent amenorrhea, due to toxicity to the ovary. The incidence of chemotherapy-induced ovarian failure depends on the regimen used, the cumulative drug doses, and the age of the patient. The rapid changes in hormone concentrations associated with chemotherapy can lead to more severe symptoms than those of natural menopause. Some reports suggest that low-dose transdermal estrogen might be safer to use in this population and is very effective for symptom relief in the general population. If such therapy is used, it should be done over the shortest time period and with the lowest effective dose. Although minimal side effects are described during the treatment period, some women experienced withdrawal bleeding 1 to 4 weeks after discontinuation of treatment with megestrol acetate; the effects of the progesterone on hot flash reductions appear to be long-lasting. In a randomized trial comparing a single intramuscular dose of medroxyprogesterone acetate to venlafaxine, medroxyprogesterone acetate was more effective and appeared to have fewer short-term toxicities (12). It should be noted, however, that there are no long-term prospective data to establish the safety of progesterone analogs agents for women with hormone-sensitive breast cancer. Nonhormonal Therapies Newer Antidepressants It is difficult to evaluate the efficacy of pharmacologic therapy for hot flashes with anecdotal reports alone, because of placebo effects. Multiple placebo-controlled trials demonstrate a 20% to 35% reduction in hot flashes with 4 weeks of placebo treatment. Venlafaxine is thought to inhibit serotonin reuptake at lower doses and to induce a more profound inhibition of norepinephrine reuptake at higher doses. A double-blind, placebo-controlled trial with 191 breast cancer survivors randomized subjects to placebo or to one of three target venlafaxine doses (37. After 4 weeks of treatment, the placebo groups had a 27% reduction in symptoms, versus 40%, 61%, and 61% reductions in the three venlafaxine groups, respectively. The side effects observed with venlafaxine include dry mouth, decreased appetite, nausea, and constipation (the latter only at doses of 150 mg/day). From these studies, it appears that venlafaxine adequately balances the symptom relief with the side effects. In contrast to these findings, the Stockholm trial of 378 participants given estrogen with or without progestin versus placebo did not show a difference in recurrence after 4 years of follow-up (8). A double-blind, randomized, placebo-controlled, crossover clinical trial demonstrated that fluoxetine reduces the incidence of hot flashes, although the reduction does not appear to be as great as that observed with venlafaxine (13,17). Two placebo-controlled, double-blinded randomized trials found that paroxetine decreased hot flashes significantly more than did a placebo (1820). Three randomized, placebo-controlled trials evaluating sertraline (50100 mg/day) for the management of hot flashes failed to reveal any substantial benefit from this drug. Escitalopram, a stereo-isomer of citalopram, was studied in 205 postmenopausal women and found to be more effective than placebo (47% vs. Two randomized, placebo-controlled clinical trials of some of these newer antidepressants (23,24) have been interpreted to be negative studies (25).
References
- Estacion M, Waxman SG, Dib-Hajj SD: Effects of ranolazine on wild-type and mutant hNav1.
- Siddiki H, Fidler J. MR imaging of the small bowel in Crohn's disease. Eur J Radiol. 2009;69:409-417.
- Capeci CM, Tejwani NC Bilateral low energy simultaneous femoral fractures in patients on long term alendronate therapy. J Bone Joint Surg Am 2009;91:2556-2561.
- Gatti RA: Ataxia-telangiectasia, Dermatol Clin 13:1-6, 1995.
- Leveillee, R., Hoey, M. Radiofrequency interstitial tissue ablation: wet electrode. J Endourol 2003;17:563-577.
- Ng CK, Kauffman EC, Lee M-M, et al: A comparison of postoperative complications in open versus robotic cystectomy, Eur Urol 57(2):274n281, 2010.
- Raynor RB. Spinal-cord compression secondary to Gaucher's disease. Case report. J Neurosurg 1962;19:902.